23.08.2020
DPP-4 blockers. DPP-4 blockers Reduce food intake and body weight
For citation:Ametov A.S., Karpova E.V. Clinical use of DPP-4 inhibitor - vildagliptin in type 2 diabetes mellitus // BC. 2010. No. 14. P. 887
In recent years, the study of the role of hormones of the gastrointestinal tract in the regulation of insulin secretion, and, consequently, in the regulation of glucose homeostasis in the human body, has been of great scientific and practical interest. Of these, the role of glucagon-like peptide 1 (GLP-1) and glucose-dependent insulinotropic polypeptide (GIP), which are called incretins, is more or less known. Incretins are hormones in the gastrointestinal tract that are released in response to food intake and stimulate insulin secretion. And their effect, leading to an increase in glucose-dependent insulin secretion by β-cells of the pancreas, was called the "incretin effect" (Fig. 1).
In recent years, the study of the role of hormones of the gastrointestinal tract in the regulation of insulin secretion, and, consequently, in the regulation of glucose homeostasis in the human body, has been of great scientific and practical interest. Of these, the role of glucagon-like peptide 1 (GLP-1) and glucose-dependent insulinotropic polypeptide (GIP), which are called incretins, is more or less known. Incretins are hormones in the gastrointestinal tract that are released in response to food intake and stimulate insulin secretion. And their action, leading to an increase in glucose-dependent insulin secretion β
-cells of the pancreas, was called the "incretin effect" (Fig. 1).
The "incretin effect" was first described by two independent research groups (McIntyre, Elrick) back in 1964 and was interpreted as a characteristic of the action of peptide hormones that are secreted by the intestinal K- and L-cells in response to food intake. It can be used to explain how insulin is stimulated in response to food intake. It should be noted that GLP-1 is currently the most studied incretin. Since the half-life of GLP-1 is very short, it cannot be used in clinical practice as a natural preparation. In this regard, it was proposed to inhibit the enzyme dipeptidyl peptidase-4 (DPP-4), which destroys the body's natural incretins.
It is well known that DPP-4 belongs to the class of serine proteases, which are abundant in the human body. The main function of the enzyme is the rapid inactivation of oligopeptides in different tissues and organs by separating two amino acids from the N-terminus. The target peptides for DPP-4 are found in the intestine - GLP-1 and GIP.
It has been studied that the DPP-4 enzyme rapidly inactivates GLP-1 and GIP immediately after their secretion in the intestine. However, upon inhibition of DPP-4, the level and activity of incretins increases, and their action is prolonged (Fig. 2).
Inhibition of DPP-4 prolongs the activity of incretins, which, in turn, increases the level of active incretins in the blood circulation. As a result, the imbalance in the ratio of insulin / glucagon is normalized: glucose-dependent insulin secretion β
-cells increases, and the secretion of glucagon α
-cells suppressed, which allows you to effectively control glycemic control against the background of a significant reduction in the risk of hypoglycemia, especially severe episodes, due to the glucose-sensitive action. Improving islet cell function leads to improved glycemic control (Figure 3).
Thus, DPP-4 inhibitors are a new class of hypoglycemic drugs, the main action of which is aimed at increasing the activity of the body's own incretins, and which, apparently, provide a better benefit / risk ratio compared to other classes of drugs for the treatment of type 2 diabetes mellitus. The data of numerous international studies have confirmed that drugs of DPP-4 inhibitors increase the level of endogenous insulin, reduce the level of glucagon in the blood plasma and suppress gluconeogenesis in the liver, reduce insulin resistance, providing full glycemic control.
Currently, DPP-4 inhibitors are an extremely promising, actively developing class of hypoglycemic drugs for the treatment of type 2 diabetes mellitus. One of the representatives of this class is vildagliptin (Galvus).
In the course of international clinical trials involving over 22 thousand patients with type 2 diabetes mellitus and impaired glucose tolerance, the efficacy of vildagliptin has been shown when used both as monotherapy and in combination with other antihyperglycemic agents. One of the main advantages of these drugs is the possibility of their use in groups of elderly patients, patients with hypertension and moderate renal dysfunction, patients of the cardiovascular risk group. Vildagliptin can be combined with any hypoglycemic drug, including insulin.
Vildagliptin monotherapy
S. Dejager et al. (2007) studied the efficacy of the drug in a placebo-controlled study lasting 24 weeks in 632 patients. After randomization in the main group, patients received vildagliptin 50 mg 2 times a day or 50-100 mg once. Compared with the initial data, the HbA1c indicators decreased by 0.7 ± 0.1%, respectively; 0.8 ± 0.2% and 0.9 ± 0.1% (Fig. 4).
In addition, the main group showed a decrease in body weight by -1.8, - 0.3 and - 0.8 kg, respectively; against the background of placebo, the weight decreased by 1.4 kg. 3 cases of mild hypoglycemia were registered in patients receiving vildagliptin.
Another study for 52 weeks compared the results of treatment with vildagliptin (50 mg 2 times / day, n \u003d 526) or metformin (1000 mg 2 times / day, n \u003d 254) in patients with type 2 diabetes mellitus at baseline mean values glycated hemoglobin 8.7%. The dynamics of glycated hemoglobin during the study was 1.0% in the main group, which was statistically significant compared to the baseline values, but without an advantage over metformin (the dynamics of the glycated hemoglobin level in the control group was 1.4%).
In addition, a study by Shweizer A. et al. , showed that at the start of drug therapy, the administration of Galvus in comparison with metformin provides a reliable, clinically significant and dose-dependent decrease in the HbA1c level by 1.1% at a dose of 50 mg 2 times a day. At the same time, the incidence of gastrointestinal side effects significantly decreased in the vildagliptin therapy group compared to metformin therapy, which was significantly less pronounced (Fig. 5). Body weight in patients of both groups remained stable with a downward trend. Thus, vildagliptin is an alternative to metformin when starting diabetes therapy.
In a study by Rosenstock J. et al. it was shown that vildagliptin is also an alternative to thiazolidinediones when starting therapy for diabetes mellitus. Galvus provided a similar 0.9% reduction in HbA1c levels as rosiglitazone. At the same time, after 24 weeks, the difference in the dynamics of body weight on therapy with rosiglitazone and vildagliptin was 2.8 kg, with an average weight increase of 1.6-1.7 kg in the rosi-glitazone therapy group and a decrease of 0.3-1. 1 kg in the vildagliptin therapy group. In addition, vildagliptin therapy is not associated with the development of edema and osteoporosis, and it can be prescribed to patients at risk of cardiovascular disease. Thus, Galvus is an alternative to thiazolidinediones when starting and continuing therapy for type 2 diabetes mellitus (Fig. 6).
Studies with the use of vildagliptin in the form of monotherapy have shown that its effectiveness increases with an increase in the initial indicators of the level of glycated hemoglobin. It was also found that the effectiveness of treatment does not depend on age and degree of obesity. On average, the level of fasting glycemia decreases by 1.0 mmol / L, postprandial - by 1.0-1.5 mmol / L.
Combination vildagliptin
with sulfonylurea preparations
In clinical trials, vildagliptin was effective and well tolerated in patients with type 2 diabetes mellitus on sulfonylurea therapy. Combined therapy with vildagliptin and glimeperide resulted in a 0.7 ± 0.1% decrease in HbA1c levels compared with glimeperide alone. In addition, it should be noted: against the background of this combination therapy, no increase in body weight was recorded in patients, which was also associated with a minimal risk of developing episodes of hypoglycemia.
Combination vildagliptin
with insulin
V. Fonseca et al. in one of their scientific works (2006) studied the effectiveness of adding vildagliptin (50 mg per day) to insulin (the average daily dose was 82 units) in 256 patients with unsatisfactory parameters of carbohydrate metabolism (the initial level of glycated hemoglobin averaged 8.4%) within 24 weeks. It is important to note that during the study period the insulin therapy regimen in patients did not change. By the end of the observation, the level of glycated hemoglobin in the study group decreased by 0.5%, in the control group (insulin in combination with placebo) - by only 0.2%. It is interesting to note that in patients aged 65 and over, the combination of insulin with vildagliptin contributed to a decrease in the level of glycated hemoglobin by 0.7%, while in the control group there was no statistically significant difference in age (Fig. 7).
It should also be noted that episodes of hypoglycemia were recorded significantly less frequently in the study group, which is probably due to an increase in the sensitivity of pancreatic a-cells to glucose (Fig. 8).
Combination vildagliptin
with metformin
It should be noted that to date, a series of studies have been carried out in which the feasibility of combination therapy of vildagliptin with metformin has been convincingly proven. Vildagliptin in combination with metformin has a synergistic effect on the synthesis and activity of GLP-1, provides effective glycemic control without the risk of hypoglycemia and weight gain.
So, already in one of the earliest randomized trials, it was demonstrated that such a combination can achieve a significant improvement in carbohydrate metabolism, and these results remained stable for a year after the completion of the study. In this study, vildagliptin at a dose of 50 mg was added to metformin therapy, which after 12 weeks led to a decrease in the level of glycated hemoglobin by 0.6% compared with the initial value (7.7%). In the control group (monotherapy with metformin), no significant changes were observed. All the next 40 weeks, against the background of combination therapy, a positive result of treatment remained, while in the control group, a progressive negative trend was observed (an increase in glycated hemoglobin by 0.066% monthly). Due to this, the difference between the groups in the level of glycated hemoglobin changed from -0.7% (12th week of observation) to -1.1% (40th week of the study).
Another study compared the efficacy of combination therapy with vildagliptin 50 mg 2 times daily. + metformin 1500 mg / day with therapy glimepiride 6 mg per day + metformin 1500 mg / day. It was shown that during the year of therapy, glycemic control was maintained equally in both treatment groups with an average decrease in HbA1c by 0.7-0.8% (with the initial HbA1c - 7.3%) (Fig. 9). After 1 year of therapy, the difference in body weight dynamics was 2.8 kg. The incidence of hypoglycemia in the vildagliptin + metformin treatment group was minimal, and there were no severe episodes at all.
It is important to note that with the combined appointment of vildagliptin and metformin, side effects from the gastrointestinal tract were observed much less frequently than with metformin monotherapy.
In recent years, evidence has emerged that metformin increases GLP-1 levels. Among the proposed mechanisms, the role of biguanides in the direct enhancement of the secretory function of intestinal L-cells, activation of transcription / translation of the proglucagon gene, a decrease in renal excretion of GLP-1, and blockade of DPP-4 are discussed.
Thus, the advantages of combined therapy of vildagliptin and metformin (additive effect on carbohydrate metabolism and complementary mechanism of action) predetermined the need for a fixed combination of these drugs. The possibility of a simultaneous effect on the key links in the pathogenesis of type 2 diabetes mellitus - insulin resistance and dysfunction of the islet cells of the pancreas - provides a high potential for this type of therapy. In the EU countries vildagliptin / metformin (Eucreas) has been used since 2007, in the Russian Federation GalvusMet was registered in March 2009. It is important to note that Galvus and GalvusMet are already widely used in more than 50 countries around the world.
Currently, the Department of Endocrinology and Diabetology with a course of endocrine surgery of GOU DPO RMAPO is studying the efficacy and safety of combination therapy of the DPP-4 inhibitor - vildagliptin (Galvus) with various hypoglycemic drugs in patients with poor control of type 2 diabetes. The first results of the study indicate that vildagliptin effectively reduces blood glucose levels both on an empty stomach and 2 hours after a meal, does not cause an increase in body weight and the development of hypoglycemia. In addition, our data convincingly prove that vildagliptin therapy provides a reliable and clinically significant decrease in glycemic variability during the day. This aspect is especially important in terms of preventing the development of the most severe macrovascular complications of diabetes. The group studying the effectiveness of the combination of vildagliptin with metformin included 20 patients (5 men and 15 women) with type 2 diabetes, mean age 43.5 ± 8.4 (from 28 to 63) years, BMI - 34.00 ± 6, 80 kg / m2, waist circumference (WT) 114.79 ± 13.47 cm, receiving metformin in a daily dose of 1500-3000 mg. Vildagliptin (Galvus) 50-100 mg / day was added to the therapy. in combination with an individually selected diet plan and physical activity regimen. The state of carbohydrate metabolism was assessed by the level of glycemia before and 2 hours after a meal, HbA1c, insulin, C-peptide, the average value of glycemia for 3 days, the duration of the period of normoglycemia, hyperglycemia, hypoglycemia for 3 days, the fluctuation of glycemia - its variability (the amount hypo- and hyperglycemic excursions, duration of excursions) according to the results of daily monitoring of glycemia. After 12 weeks of therapy with vildagliptin 50-100 mg / day. and metformin 1500-3000 mg / day. reliable dynamics of all indicators of carbohydrate metabolism was achieved: glycemia before meals decreased from 10.8 ± 0.81 to 6.2 ± 0.95 mmol / l (p<0,001), постпрандиальная гликемия с 14,6±1,2 ммоль/л до 8,5±0,98 ммоль/л (p<0,001), HbA1c с 8,23±0,81 до 6,64±0,64% (p<0,001), среднее значение гликемии в течение 3 суток снизилось с 9,24±1,94 до 7,64±2,26 ммоль/л (p<0,001), продолжительность пе-риода нормогликемии увеличилась с 26,33±10,8 до 57,71±14,64% (p<0,001), гипергликемии с 73,67±10,8 до 41,86±14,64% (p<0,001), по данным результата суточного мониторирования гликемии достоверной динамики вариабельности гликемии и развития эпизодов гипогликемии не зафиксировано. Отмечалась положительная динамика массы тела и ОТ. Через 12 недель на фоне коррекции образа жизни и применения комбинированной терапии масса тела снизилась с 96,84±16,14 до 87,63±14,3 кг (p<0,001), ОТ уменьшилась с 114,79±13,47 до 105,6±13,0 см (p<0,001). Побочных эффектов не наблюдалось, биохимические параметры оставались в норме. Отмечалась хорошая переносимость, а также, что немаловажно - улучшение качества жизни пациентов. Таким образом, в нашем исследовании вилдаглиптин в комбинированной терапии с метформином на фоне соблюдения плана питания и режима физической активности показал высокую эффективность в компенсации углеводного обмена, при этом вариабельность гликемии оставалась без динамики.








Literature
1. Fonseca V, at al. Addition of vildagliptin to insulin improves glycaemic control in type 2 diabetes. Diabetologia. 2007; 50: 1148-1155.
2. King H, Aubert RE & Herman WH. Global burden of diabetes, 1995-2025: prevalence, numerical estimates, and projections. Diabetes Care 1998; 1414-1431.
3. Niskanen L, Turpeinen A, Penttila I, Uusitupa MI. Hyperglycemia and compositional lipoprotein abnormalities as predictors of cardiovascular mortality in type 2 diabetes: a 15-year follow-up from the time of diagnosis. Diabetes Care 1998; 21 (11): 1861-1869.
4. Manson JE, Colditz GA, Stampfer MJ, et al. A prospective study of maturity-onset diabetes mellitus and risk of coronary heart disease and stroke in women. Arch Intern Med. 1991; 151: 1141-1147.
5. Garber A. G., et al. Efficacy and Tolerability of Vildagliptin Added to a Sulfonylurea in Patients with Type 2 Diabetes. Presented at ADA, 22-26 June 2007 (Abstract 501-P).
6. Fonseca V., Dejager S., Albrecht S. et al. Vildagliptin as add-on to insulin in patients with type 2 diabetes (T2DM). Diabetes 2006; 55 (suppl 1): A111.
7. Neaton JD, Wentworth DN, Cutler J, Stamler J, Kuller L Risk factors for death from different types of stroke. Multiple Risk Factor Intervention trial Reasearch Group. Ann Epidemiol. 1993; 3: 493-499.
8. Stratton JM, Adler AI, Neil AW, et al. Association of glycaemia with macrovascular and microvascular complications of type 2 diabetes (UKPDS 35): prospective, observational study. BMJ. 2000; 321: 405-412.
9. Croxtall J.D., Keam S.J. Vildagliptin: a review of use in the management of type 2 diabetes mellitus. Drugs 2008; 68 (16): 2387-2409.
10. Halimi S., Schweizer A., \u200b\u200bMinic B. et al. Combination treatment in the management of type 2 diabetes: focus on vildagliptin and metformin as a single tablet. Vascular Health and Risk Management 2008; 4 (3): 481-492.
Features:: a relatively new class of antidiabetic drugs. Drugs in this group extend the "life" in the body of special substances that stimulate the production of insulin after eating. When a person is not eating, these remedies do not work, and therefore the risk of a sharp drop in blood glucose levels is significantly reduced.
Most common side effects: allergic reactions.
The main contraindications: individual intolerance, type 1 diabetes mellitus, diabetic ketoacidosis, pregnancy, lactation, age up to 18 years.
Important information for the patient:
- The drugs are usually prescribed for a long time, often as part of a combination treatment.
- Unlike many other drugs for the treatment of diabetes mellitus, they are well tolerated. The incidence of adverse events in clinical trials was comparable to that with placebo.
- Most effective for newly diagnosed type 2 diabetes and in the early years of the disease.
- Applied regardless of food intake once a day, except for vildagliptin (1-2 times a day).
| Trade name of the drug | Price range (Russia, rub.) | Features of the drug that are important for the patient to know |
|---|---|---|
| Active substance: Sitagliptin | ||
| Januvia (Merck Sharp and Dome) |
2046-3350 | The first drug in this group has been fairly well studied today. In combination with insulin and sulfonylurea derivatives, it has not been studied, therefore, joint administration is not recommended. |
| Active substance: Vildagliptin | ||
| Galvus (Novartis) |
718,06-900,55 | A mildly acting drug that can be combined with any other antidiabetic agents, including as a third antidiabetic agent in case of insufficient effectiveness of treatment with sulfonylureas and metformin or insulin and metformin. Contraindicated in hereditary galactose intolerance, lactase deficiency and other sugars. Not recommended for use in patients with severely impaired liver function. |
| Active substance: Saxagliptin | ||
| Onglisa (Bristo-Myers Squibb, Astra-Zeneca) |
1460-2365 | A powerful drug. It can be used in conjunction with most other antihyperglycemic drugs, however, together with sulfonylurea derivatives, it should be used with caution. Contraindicated in hereditary galactose intolerance, lactase deficiency and other sugars. It is prescribed with caution in moderate and severe renal failure, as well as in elderly patients. |
| Active substance: Linagliptin | ||
| Trajenta (Beringer Ingelheim) |
1350-2310 | A new highly selective drug that combines well with other antidiabetic drugs. May be the agent of choice in patients with impaired renal and hepatic function. |
Remember, self-medication is life-threatening, consult your doctor for advice on the use of any medications.
The number of patients with type 2 diabetes mellitus (DM) is growing steadily and has almost reached epidemic proportions, and the incidence continues to grow worldwide. Micro- and macrovascular complications of type 2 diabetes have an adverse effect on the quality and duration of life of patients and are associated with significant health care costs.
Currently, in addition to lifestyle modification, various classes of glucose-lowering drugs are used to lower blood glucose levels. In the USA and European countries, metformin is recommended as the first-line drug for the treatment of patients with type 2 diabetes, due to its effectiveness and low cost. However, diabetes is a progressive disease and over time most patients will need multiple medications to achieve adequate glycemic control. Among them, in a recent joint resolution of the American Diabetes Association and the European Association for the Study of Diabetes, the following agents were proposed: sulfonylureas, thiazolidinediones, dipeptidyl peptidase-4 (DPP-4) inhibitors, glucone-like peptide-1 (GLP-1) receptor agonists, and insulin. It is possible to use different combinations of hypoglycemic agents, while an individual selection of the therapy regimen is recommended and the choice will largely be determined by factors such as patient preferences, tolerance, frequency of administration and cost of drugs. Thus, the use of a number of hypoglycemic agents is associated with the risk of developing adverse events, in particular hypoglycemia, weight gain, gastrointestinal discomfort and fluid retention, which may limit their use in the long term. It should be noted that the use of a number of glucose-lowering drugs is limited with a decrease in renal function.
 In addition, the pathophysiological process underlying the development of diabetes mellitus is not limited to impaired insulin secretion and insulin resistance. According to DeFronzo R.D. (2009), in addition to muscle tissue, liver and β-cells ("the ruling triumvirate"), adipocytes (activation of lipolysis), the gastrointestinal tract (deficiency of incretins or resistance to their action) play an equally important role in the pathogenesis of type 2 diabetes. α-cells of the pancreas (overproduction of glucagon), kidneys (increased glucose reabsorption) and the brain (increased appetite due to imbalance of neurotransmitters against the background of insulin resistance). In general, all these tissues and organs form an ominous octet, which predetermines more stringent requirements for the tactics of treating type 2 diabetes:
In addition, the pathophysiological process underlying the development of diabetes mellitus is not limited to impaired insulin secretion and insulin resistance. According to DeFronzo R.D. (2009), in addition to muscle tissue, liver and β-cells ("the ruling triumvirate"), adipocytes (activation of lipolysis), the gastrointestinal tract (deficiency of incretins or resistance to their action) play an equally important role in the pathogenesis of type 2 diabetes. α-cells of the pancreas (overproduction of glucagon), kidneys (increased glucose reabsorption) and the brain (increased appetite due to imbalance of neurotransmitters against the background of insulin resistance). In general, all these tissues and organs form an ominous octet, which predetermines more stringent requirements for the tactics of treating type 2 diabetes:
1) to correct multiple pathophysiological disorders, it is necessary to use combined drug therapy;
2) therapy should be aimed not only at reducing glycated hemoglobin (HbA1c), but also at all known pathogenetic factors of type 2 diabetes;
3) treatment should be started as early as possible in order to prevent or slow down the progression of β-cell deficiency, which is already observed at the NTG stage.
A classic dysfunction of the pancreas in type 2 diabetes is the absence of the first phase of insulin secretion with intravenous or oral glucose administration. In addition, in patients with type 2 diabetes, there is a decrease in the reaction of β-cells in response to other secretagogues (arginine, secretin, etc.), suppression of the pulsating nature of insulin secretion, a decrease in the maximum secretory reserves, and hyperproduction of proinsulin. To date, far from all the mechanisms of these violations have been clarified. Presumably, age factors, hereditary predisposition, insulin resistance, lipo- and glucose toxicity, amyloid accumulation, the influence of pro-inflammatory cytokines, and impaired incretin effects play a dominant role in the development of functional and structural changes in β-cells.
Taking all this into account, clinicians pin great hopes on the fundamentally new antihyperglycemic agents developed in recent years, the mechanism of action of which is closely related to the effects of incretins.
Synthesis, secretion and biological effects of incretins
 It has long been suggested that substances that can lower blood glucose levels are synthesized in the gastrointestinal tract (GIT). In 1906 B. Moore demonstrated that substances excreted from the duodenum can reduce the concentration of glucose in urine. These substances were named "incretins" (incretin - INtestinal seCRETion of INsulin). The development of radioimmunological research methods has confirmed the hypothesis of the existence of an enteroinsular relationship. As it turned out, the level of insulin is significantly higher with oral glucose than with intravenous ("incretin effect"). Up to 70% of the insulin released in response to oral glucose load is due to the influence of incretins - hormones produced in the gastrointestinal tract during the digestion of food. The first incretin to be identified suppressed the secretion of hydrochloric acid in the stomach in dogs, which formed the basis of its name - gastric inhibitory polypeptide (GIP). Later it was found that LIP is capable of increasing insulin secretion in both animals and humans. Since the blockade of hydrochloric acid production was observed only against the background of pharmacological doses of the hormone, and the effect of incretins against the background of physiological ones, the GIP was renamed the glucose-dependent insulinotropic polypeptide (GIP). Currently, both terms are used interchangeably.
It has long been suggested that substances that can lower blood glucose levels are synthesized in the gastrointestinal tract (GIT). In 1906 B. Moore demonstrated that substances excreted from the duodenum can reduce the concentration of glucose in urine. These substances were named "incretins" (incretin - INtestinal seCRETion of INsulin). The development of radioimmunological research methods has confirmed the hypothesis of the existence of an enteroinsular relationship. As it turned out, the level of insulin is significantly higher with oral glucose than with intravenous ("incretin effect"). Up to 70% of the insulin released in response to oral glucose load is due to the influence of incretins - hormones produced in the gastrointestinal tract during the digestion of food. The first incretin to be identified suppressed the secretion of hydrochloric acid in the stomach in dogs, which formed the basis of its name - gastric inhibitory polypeptide (GIP). Later it was found that LIP is capable of increasing insulin secretion in both animals and humans. Since the blockade of hydrochloric acid production was observed only against the background of pharmacological doses of the hormone, and the effect of incretins against the background of physiological ones, the GIP was renamed the glucose-dependent insulinotropic polypeptide (GIP). Currently, both terms are used interchangeably.
In the course of experiments with immunoneutralization of the GIP, it was noticed that the incretin effect, although somewhat reduced, does not completely disappear. In addition, despite the normal GIP content, after resection of the ileum in humans, a decrease in the insulin response to oral glucose administration is observed.
The discovery of the second incretin, glucagon-like peptide-1 (GLP-1), which is a product of the proglucagon gene, made it possible to gain a more complete understanding of the mechanisms of regulation of postprandial insulin secretion.
Glucagon-like peptide-1
The proglucagon gene is expressed by α cells in the pancreas, L cells of the small intestine, and neurons in the brain stem and hypothalamus. The main product of this gene, proglucagon, which includes 160 amino acids, undergoes post-translational tissue-specific processing under the influence of proconvertase 2 and proconvertase 1/3 (Fig. 1). As a result of the cleavage of proglucagon in the pancreas, glucagon, glycentin-linked pancreatic peptide (GSPP), intermediate peptide-1, and the main proglucagon fragment are formed. The processing of proglucagon in intestinal L-cells and the brain leads to the formation of glucagon-like peptides-1 and -2, glycentin, an intermediate peptide and oxyntomodulin.

Figure: 1. Post-translational processing of proglucagon in the pancreas, intestines and brain
Glucagon is the most important counterinsular hormone that regulates the production of glucose by the liver by activating glycogenolysis and gluconeogenesis, and suppressing glycolysis. The physiological role of glucagon is to maintain normal fasting glucose homeostasis and is most evident in hypoglycemic conditions. In patients with type 2 diabetes, the level of the hormone is usually steadily increased.
Oxyntomodulin and glucagon-like pepid-2 (GLP-2) suppress the secretion of hydrochloric acid in the stomach and slow down its motility, increase the utilization of glucose in the intestine, and enhance the feeling of satiety. In addition, oxyntomodulin increases the activity of pancreatic enzymes and is involved in the regulation of heart rate. GLP-2 stimulates the proliferation of intestinal cells and neurons in the brain, suppresses their apoptosis, and also reduces bone resorption.
The physiological significance of glycentin has not been definitively determined; according to experimental studies, it is able to have a positive effect on the trophism of the small intestine in rodents. At the moment, the biological effects of intermediate peptides-1, -2, glycentin-linked pancreatic peptide and the main fragment of proglucagon have not been specified.
Glucagon-like peptide-1, secreted by the L-cells of the ileum and colon, performs many functions in the body, the most important of which is to enhance and maintain the secretory function of the pancreas. The hormone level in patients with diabetes mellitus is reduced, and a defect in the secretion of GLP-1 was found in patients with the initial manifestations of type 2 diabetes and even in those with prediabetes (Fig. 2).

Figure: 2. Decreased GLP-1 secretion in persons with carbohydrate metabolism disorders.
GLP-1 receptors belonging to the family of G-protein coupled receptors (seven transmembrane domains) are localized on α-, β-, and δ-cells of the islets of Langerhans, as well as in the lungs, heart, kidneys, skin, and gastrointestinal tract , the brain.
The period of stay of the hormone in the active form - GLP-17-36 or GLP-17-37 is only about two minutes, then it undergoes rapid destruction with the formation of metabolites GLP-19-36 and GLP-19-37 under the action of the enzyme dipeptidyl peptidase-4 ( DPP-4). DPP-4 is present in many organs and tissues, including the kidneys, lungs, liver, intestines, spleen, pancreas, adrenal glands, and the central nervous system. In addition to the membrane-bound form, DPP-4 also exists as a soluble protein circulating in the bloodstream.
As a result of inactivation, on average, only 25% of newly secreted active molecules of glucagon-like peptide-1 leave the gastrointestinal tract, another 45-50% is destroyed in the liver. Thus, only 10–15% of intact molecules are present in the systemic circulation (Fig. 3).

Figure: 3. Secretion and inactivation of glucagon-like peptide-1 in the gastrointestinal tract
Digestible food, which is predominantly rich in fats and carbohydrates, is the main stimulus for GLP-1 secretion. The production of the hormone can increase both under the influence of mixed food, and under the influence of its individual components - glucose and other sugars, fatty acids, amino acids, fiber.
As a result of the interaction of GLP-1 with the receptor, adenylate cyclase is activated and the level of cyclic adenosine-3 ', 5'-monophosphate (cAMP) increases, followed by an increase in the activity of protein kinase A (PKA) and metabolic proteins associated with cAMP (POAC). This, in turn, leads to increased insulin secretion through the following molecular mechanisms:
1) blockade of ATP-dependent potassium channels with subsequent depolarization of the cell membrane;
2) an increase in the intracellular content of calcium ions due to its influx through voltage-dependent calcium channels;
3) blockade of voltage-dependent potassium channels responsible for repolarization of the cell membrane, which, accordingly, leads to an increase in the duration of the action potential;
4) mobilization of intracellular calcium stores;
5) stimulation of ATP synthesis in mitochondria, which is accompanied by: a) further depolarization of the cell membrane by blockade of ATP-dependent potassium channels, b) stimulation of exocytosis of insulin-containing granules;
6) an increase in the pool of insulin-containing granules, ready for immediate secretion, located in close proximity to the cell membrane, by attracting granules from the reserve pool located in the deep cytoplasm (Fig. 4).
cAMP - cyclic adenosine-3 ', 5'-monophosphate
PKA - protein kinase A
AC - adenylate cyclase
POAC - metabolic proteins associated with cAMP
IF3 - inositol-3-phosphate
Figure: 4. The mechanism of increasing insulin secretion under the action of glucagon-like peptide-1
The insulinotropic activity of GLP-1 is determined by the level of glycemia. The threshold level for the onset of action is about 70 mg / dl, a clinically significant increase in insulin secretion is recorded at a glucose concentration within 110 mg / dl, while sulfonylureas can depolarize the cell membrane even at low glycemic values.
GLP-1 takes part in the transcription of the insulin gene, ensures the stability of its mRNA, and regulates the process of insulin biosynthesis. Thus, GLP-1 replenishes the stores of insulin in β-cells and prevents their premature depletion. In addition, GLP-1 increases the expression of type 2 glucose transporters and hexokinase in β-cells, thereby restoring their sensitivity to glucose.
The most important property of GLP-1 is the experimentally proven ability to suppress β-cell apoptosis, enhance their proliferation and neogenesis from progenitor cells located in the pancreatic ducts. Presumably, GLP-1 affects the growth and differentiation of islet cells, the preservation of their mass primarily by increasing the expression of the pancreato-duodenal home domain of gene-1 ( PDX-1- pancreatic duodenal homeobox gene 1), which ensures the development of the pancreas even in the embryonic period. Mutations PDX-1 accompanied by the development of the agenesis of the pancreas.
GLP-1 also makes a significant contribution to the regulation of carbohydrate metabolism by suppressing glucagon secretion, thereby reducing the production of glucose by the liver. It is most likely that the effect on glucagon production is mediated by an increase in somatostatin level under the influence of GLP-1; evidence of a direct inhibitory effect is currently insufficient.
By acting on the afferent fibers of the vagus nerve, glucagon-like peptide-1 slows down the rate of gastric emptying, increases its volume and suppresses the secretion of hydrochloric acid. Thus, the hormone acts as an ileal-intestinal brake - an inhibitory mechanism due to which the distal intestine regulates the overall transit of nutrients through the gastrointestinal tract. Slowing down the rate of food evacuation helps to reduce the level of postprandial glycemia.
The introduction of GLP-1 is accompanied by suppression of appetite and a decrease in body weight in animals and humans, which is due to the central and peripheral effects of the hormone.
In rats, central (intraventricular) administration of GLP-1 leads to a dose-dependent decrease in the volume of food intake, this effect is blocked by the use of the GLP-1 receptor antagonist exendin 9-39. The central anorexigenic action is realized at least at two levels: 1) the interaction of the hormone with its receptors in the arcuate nuclei of the hypothalamus promotes the activation of neurons producing proopiomelanocortin and cocaine-amphetamine-regulated transcript; 2) GLP-1 receptors, located in the amygdala, are responsible for the development of symptoms of general malaise and disturbances in taste.
To date, it is not entirely clear how the decrease in appetite occurs with intravenous or subcutaneous administration of glucagon-like peptide-1 (this effect is clearly seen in healthy volunteers, as well as in patients with obesity and type 2 diabetes). The most likely mechanism seems to be a slowdown in gastric motility and an increase in its volume. On the other hand, GLP-1 molecules are able to overcome the blood-brain barrier; thus, the direct role of the hypothalamic arcuate nuclei in the realization of the anorexigenic effects of the hormone, even with its peripheral administration, is not completely excluded.
Recently published reports on the beneficial effects of GLP-1 on the cardiovascular system are noteworthy. Hormone receptors are found in the myocardium. In animals, under the influence of GLP-1, there is an improvement in the left ventricular and systemic hemodynamics, the zone of experimentally induced ischemia decreases. Intravenous administration of the hormone in patients with type 2 diabetes leads to the normalization of endothelial function; in patients with myocardial infarction - to the restoration of left ventricular function, a reduction in the period of hospitalization and in-hospital mortality.
Glucose-Dependent Insulinotropic Polypeptide
GIP is synthesized and secreted in enteroendocrine K-cells, mainly localized in the duodenum and proximal jejunum. The physiological stimulant of secretion is digestible food rich in fats and carbohydrates. The active form of the hormone is rapidly destroyed under the influence of DPP-4, the half-life is about seven minutes in a healthy person and five minutes in type 2 diabetes patients. The molecular mechanisms by which GIP stimulates insulin secretion in β-cells are similar to glucagon-like peptide-1 and include an increase in cAMP content, blockade of ATP-dependent potassium channels, an increase in calcium ion content, and stimulation of exocytosis. Like GLP-1, glucose-dependent insulinotropic polypeptide enhances β-cell proliferation and suppresses their apoptosis.
At the same time, in contrast to glucagon-like peptide-1, GIP does not affect glucagon secretion, gastric motility and satiety.
GIP receptors are present in the hippocampus and olfactory bulbs. Presumably, the GIP is involved in the proliferation of progenitor cells in the corresponding parts of the brain.
In adipocytes, the hormone stimulates the synthesis and esterification of free fatty acids, increases the synthesis of lipoprotein lipase and inhibits glucagon-stimulated lipolysis.
GIP receptors are found on osteoblasts and osteoclasts. In rodents, the inhibitory effect of the hormone on bone resorption was noted. In humans, short-term administration of the hormone has no significant effect on bone metabolism; the therapeutic potential for chronic use has not yet been studied.
Molecular mechanisms of incretin effect
As noted above, the production of insulin in response to oral glucose load is significantly higher than to its intravenous administration. How glucose in the intestinal lumen enhances the secretion of incretins became known only in 2007 thanks to the works of Jang H.J. and Margolskee R.F. et al.
Man is able to distinguish five different types of tastes: sweet, bitter, salty, sour and umami (“meaty”, caused by a number of amino acids, in particular, monosodium glutamate). Taste plays an important role in deciding whether food is acceptable or not. The perception of taste protects the body from potential poisons and toxins (bitter), spoiled food (sour), determines the preference for high-calorie (sweet), sodium-enriched (salty) and protein (umami) foods.
The function of taste recognition is performed by the taste receptors - specialized epithelial cells with neuron-like properties, located on the taste buds of the surface of the tongue and soft palate. The innervation of the taste buds is carried out by the facial and vagus nerves. For sweet components, the signaling cascade begins with the activation of G-protein coupled receptors T1R2 T1R3, forming a heterodimer. A key component of intracellular signal transduction is the G-protein specific for taste cells, gastducin (gustducin), which, upon activation, breaks down into three subunits: α-gastducin, Gβ3 and Gγ13. The β- and γ- subunits activate phospholipase Cβ2 with subsequent stimulation of inositol-3-phosphate (IF3) and an increase in the content of intracellular calcium.
Studies carried out in recent years have shown a similarity in the structure of taste cells of the tongue and enteroendocrine cells of the intestine. As it turned out, it is the T1R2 T1R3 receptor that recognizes the sweet taste that is the sensor of glucose in the intestine, and the secretion of GLP-1 and GIP is mediated by the activation of the taste G-protein gastducin, which is contained not only in specific cells of the oral cavity, but also in enteroendocrine L- and K -cells. In the experiment, in mice lacking the gastducin gene, along with the pathology of the taste analyzer, there was a pronounced decrease in GLP-1 secretion and corresponding disorders of carbohydrate metabolism.
Incretin-targeted therapy
Given the rapid inactivation of GLP-1 under the influence of dipeptidyl peptidase-4, there are two approaches to using the incretin pathway to treat hyperglycemia in people with type 2 diabetes:
1) the use of incretin mimetics or agonists of GLP-1 receptors resistant to destruction of LGG-4 (for example, exenatide, lixisenatide and liraglutide);
2) the use of DPP-4 inhibitors, which increase the plasma half-life of endogenous GLP-1 (for example, sitagliptin, vildagliptin, saxagliptin and linagliptin).
As shown in the meta-analysis by Amori R.E. et al. (2007), despite the differences in the modes of administration (subcutaneous or oral), as well as in the concentration of GLP-1 induced by the administration of incretin-mimetics or DPP-4 inhibitors, both classes of drugs are practically equivalent in terms of their antihyperglycemic effect. Thus, it is possible that such a pronounced effect of DPP-4 inhibitors on islet cell function is associated not only with the activation of glucagon-like peptide-1, but also with other substrates of dipeptidyl peptidase-4, including GIP.
Inhibition of the DPP-4 enzyme solves a number of problems associated with the use of GLP-1 analogues. In particular, this concerns the mode of administration (injection) and such undesirable side effect as nausea.
Inhibitors of dipeptidyl peptidase-4 are an extremely promising, actively developing class of glucose-lowering drugs. The group's first DPP-4 inhibitor, sitagliptin, was approved in 2006; it was followed by vildagliptin (in many countries since 2007), saxagliptin (in 2009), alogliptin (in 2010 only in Japan, since 2013 - worldwide) and linagliptin (in 2011). Tenelagliptin, anagliptin and hemagliptin are in clinical trials. The unique mechanism of action allows the use of drugs of this group both as monotherapy and in combination with traditional drugs. They are prescribed regardless of food intake, in general, they are well tolerated, in the framework of monotherapy they reduce the level of glycated hemoglobin by 0.5 - 1.06%, are characterized by a low risk of developing hypoglycemic conditions and a potentially protective effect on beta cells. These drugs have a neutral effect on body weight, which is important, since its control in type 2 diabetes is the second most important parameter (after HbA1c). DPP-4 inhibitors have a number of advantages over other hypoglycemic drugs and can be considered as second-line drugs if metformin therapy is ineffective. However, their use in the early stages of the disease in the presence of contraindications and / or intolerance to metformin brings tangible benefits. It should be noted the high cardiovascular potential of DPP-4 inhibitors as drugs that provide effective glycemic control and have a favorable cardiovascular profile.
As the number of DPP-4 inhibitors on the pharmaceutical market increases, potential pharmacological differences between different members of the group become important in choosing the drug that is best suited for a particular patient. Despite the general mechanism of action, these drugs exhibit significant structural heterogeneity, which can lead to different pharmacological properties. At the pharmacokinetic level, DPP-4 inhibitors have important differences, including half-life, systemic exposure, bioavailability, protein binding, metabolism, presence of active metabolites, and excretion pathways. These differences may be significant, especially in patients with renal or hepatic impairment, and when considering combination therapy. At the pharmacodynamic level, the available data show a similar efficacy of all drugs in terms of antihyperglycemic effect, both as monotherapy and in combination with drugs from other groups, a similar neutral effect on body weight, and a comparable safety and tolerability profile.
Chemical structure
Representatives of the DPP-4 inhibitor class differ in molecular structure, despite the fact that they are all small (Fig. 5).
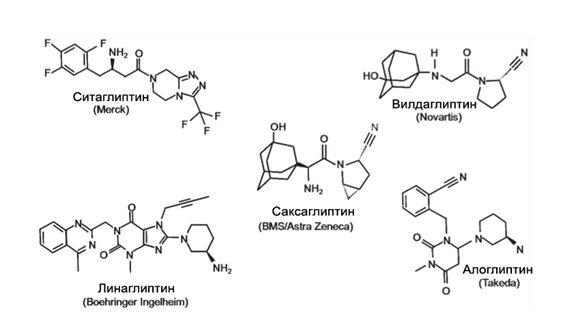
Figure: five. Chemical structure of DPP-4 inhibitors.
As a therapeutic class, DPP-4 inhibitors include a heterogeneous group of compounds that can nevertheless be divided into those that mimic the dipeptide structure of DPP-4 substrates and those that are not peptidomimetic. Such drugs as sitagliptin (based on a β-amino acid), as well as vildagliptin and saxagliptin, which are nitrile-containing inhibitors, belong to the first group (peptidomimetic DPP-4 inhibitors), while alogliptin (modified pyrimidinedione) and linagliptin (developed on based on xanthine) are representatives of the second group (Fig. 5, Table 2).
All DPP-4 inhibitors reversibly bind competitively to the active site of the enzyme, demonstrating high affinity for the enzyme. However, there are differences in the way it interacts with the enzyme. Sitagliptin, alogliptin and linagliptin form a non-covalent bond in the DPP-4 catalytic center, while vildagliptin and saxagliptin bind to the active center of the enzyme via a covalent bond. The covalent bond leads to the formation of a stable enzyme-inhibitor complex, characterized by a low dissociation rate, which allows the inhibitor to remain active even after the drug is removed. This explains why vildagliptin and saxagliptin exert their effects for a longer time than their half-life would suggest.
Table 2. Chemical structure, metabolism and routes of elimination of DPP-4 inhibitors [according to C.F. Deacon, 2011].
|
Inhibitor |
Chem. structure |
Metabolism |
Excretion path |
|
Sitagliptin |
Β-amino acid based |
Not metabolized |
Renal (~ 80% unchanged) |
|
Vildagliptin |
Cyanopyrrolidine |
Hydrolysis with the formation of inactive metabolites (P450 independent pathway) |
Renal (22% unchanged, 55% as primary metabolites) |
|
Saxagliptin |
Cyanopyrrolidine |
It is metabolized in the liver with the formation of active metabolites (via P450 3A4 / 5 |
Renal (12 - 29% unchanged, 21 - 52% as metabolites) |
|
Alogliptin |
Modified pyrimidinedione |
Not metabolized |
Renal (\u003e 70% unchanged) |
|
Linagliptin |
Xanthine based |
Not metabolized |
Hepatic (\u003e 70% unchanged,< 6 % через почки |
Power and efficiency of DPP-4 inhibition
A study that compared drugs directly under identical experimental conditions showed that all five inhibitors showed similar efficacy (i.e. maximum effect) in inhibiting DPP-4 in vitro, but differences in potency (i.e. amount required for inhibition of the compound IC 50 \u003d ~ 1 nmol for linagliptin against 19, 62, 50 and 24 nmol for sitagliptin, vildagliptin, saxagliptin and alogliptin, respectively). Differences were also noted with respect to the half-life of the drugs. Vildagliptin and saxagliptin are cleared from plasma relatively quickly, while sitagliptin, alogliptin, and linagliptin have a longer life span (Table 3). These differences are reflected in therapeutic doses (which range from 5 mg for saxagliptin and linagliptin to 100 mg for sitagliptin) and dosing frequency (once daily for most, twice daily for vildagliptin, Table 3).
Nevertheless, despite the differences in potency, when used in therapeutic doses, the effect of inhibitors in terms of the degree of inhibition of DPP-4 in vivo is generally similar. More than 90% inhibition is achieved within 15 minutes after ingestion, with 70-90% inhibition maintained for 24 hours after dosing (Table 3). In the case of vildagliptin, despite a decrease in plasma DPP-4 inhibition to almost 50% after 24 hours at a dose of 50 mg, a therapeutic twice daily dosing regimen maintains\u003e 80% inhibition of plasma DPP-4 over the entire 24-hour period. However, it should be noted that inhibition of plasma DPP-4 was assessed ex vivo (i.e., in post-in vivo blood plasma samples) and was not usually corrected for sample dilution for analysis. Therefore, the present in vivo inhibition of DPP-4 is likely to be higher than measured values \u200b\u200bsuggest.
Table 3. Half-life, dosage and effectiveness of dipeptidyl peptidase (DPP-4) inhibition [by C.F. Deacon, 2011]
|
Inhibitor |
Connection t 1/2 (h) |
Dosage |
Inhibition DPP -4 * |
|
Sitagliptin |
100 mg per day |
Max ~ 97%; \u003e 80% after 24 h of admission |
|
|
Vildagliptin |
50 mg 2 times a day |
Max ~ 95%; \u003e 80% after 12 hours of admission |
|
|
Saxagliptin |
2 - 4 (unchanged), 3 - 7 (metabolites) |
5 mg per day |
|
|
Alogliptin |
25 mg per day |
Max ~ 90%; ~ 75% after 24 hours of admission |
|
|
Linagliptin |
5 mg per day |
Max ~ 80%; ~ 70% after 24 hours of admission |
* DPP-4 activity was measured in blood plasma ex vivo, not adjusted for sample dilution during analysis.
Selectivity
DPP-4 is a member of the protease family, two of which (DPP-8 and 9) have shown preclinical toxicity and suppression of T-cell activation and proliferation in several (but not all) studies. In order to minimize any potential side effects, inhibitors intended for therapeutic use should be evaluated in this regard (Table 4). Thus, sitagliptin and alogliptin can be described as highly selective; they have essentially not demonstrated in vitro inhibitory activity against other members of the dipeptidyl peptidase family Vildagliptin and saxagliptin are less selective for inhibiting DPP-8/9 in vitro, although whether this is relevant in vivo is debatable since DPP-8/9 is located intracellularly. Linagliptin, being highly selective for DPP-8/9, is less selective for fibroblast-activating protein-α (FAP-α) / seprase. FAP-α is an intracellular enzyme that is usually present in normal adult tissues (although it is expressed in stromal fibroblasts and upregulated during tissue remodeling). However, the extent of any in vivo inhibition of FAP-α by therapeutic doses of linagliptin in humans has not been described.
None of the inhibitors have any significant inhibitory activity against the CYP 450 enzyme system.
Table 4. In vitro selectivity of DPP-4 inhibitors (fold selectivity for DPP-4 versus other enzymes) [according to C.F. Deacon, 2011]
|
Inhibitor |
Selectivity |
|||||
|
Sitagliptin |
||||||
|
Vildagliptin |
moderate |
|||||
|
Saxagliptin |
moderate |
No data |
||||
|
Alogliptin |
||||||
|
Linagliptin |
moderate |
|||||
|
QPP - inactive cellular proline dipeptidase; PEP, prolyl endopeptidase; FAP-α - fibroblast-activating protein-α |
||||||
Suction
All DPP-4 inhibitors exist in oral form and are rapidly absorbed, with significant inhibition of plasma DPP-4 observed within 5 minutes after ingestion. Oral bioavailability in humans is generally high (~ 87% for sitagliptin, ~ 85% for vildagliptin, and ~ 67% for saxagliptin), although it is slightly lower for linagliptin (~ 30%).
Distribution
The data show that the volume of distribution of different inhibitors in humans is greater than the total amount of fluid (~ 70 L for vildagliptin, 198 L for sitagliptin, 300 L for alogliptin, 2.7 L / kg for saxagliptin, and ~ 1100 L for linagliptin), suggesting that these compounds are widely distributed in body tissues. However, while their chemical structure suggests a low likelihood that they will freely cross the cell membrane, there is not enough information for sitagliptin, alogliptin, and linagliptin on whether they actually cross the cell membrane or not. The permeability of the inner membrane for saxagliptin is very low, and neither the drug itself nor its main metabolite (BMS-510849) are known substrates for cell transporters (including multidrug-resistant P-glycoprotein, Pgp). There is indirect evidence that vildagliptin is able to cross the cell membrane. Vildagliptin has been reported to inhibit DPP-8/9 in vivo in rats at very high doses (\u003e 600 times human). Since DPP-8/9 is located in the cytosol, it can be assumed that vildagliptin has access to the intracellular space, but it remains unclear whether this occurs in humans at therapeutic doses.
In plasma, most inhibitors show low reversible protein binding (38% for sitagliptin, 10% for vildagliptin and negligible for saxagliptin). In contrast, linagliptin actively binds to plasma proteins, depending on the concentration, and it was calculated that in a therapeutic dose (5 mg), most of the drug is in a protein-bound form (primarily DPP-4).

Figure 6. Concentrations of freely circulating DPP-4 inhibitors.
The low concentration of the substance in free form, combined with high selectivity to DPP-4, allows avoiding inappropriate influence. * - The calculated value for saxagliptin is underestimated, since the effect of its main active metabolite in plasma is 2-7 times higher than that of the parent substance.
Preclinical studies have shown that the highest drug concentrations were found in the intestines, kidneys, and liver, which are also tissues with the highest DPP-4 expression. Available information indicates that very low levels of inhibitors are found in the brain (saxagliptin and its major metabolite, vildagliptin and linagliptin), suggesting that these compounds cannot cross the blood-brain barrier. However, it turned out that they freely penetrate the placenta (saxagliptin, vildagliptin and sitagliptin).
Metabolism
Sitagliptin, alogliptin, and linagliptin are not significantly metabolized in vivo in humans; about 80% of the dose is excreted unchanged as the parent compound (Table 2). For sitagliptin, limited metabolism results in six trace metabolites (each accounting for less than 1% to 7% of sitagliptin-bound plasma material), with in vitro studies indicating that the main enzyme responsible for this is CYP3A4 with less contribution from CYP2C8 ... Three of these metabolites (M1, M2 and M5) are active, but do not significantly affect the pharmacodynamic profile of sitagliptin due to the combination of low plasma concentration and low affinity for DPP-4. For alogliptin, the parent molecule is\u003e 80% alogliptin bound plasma material, and two small metabolites, N-demethylated (active) and N-acetylated (inactive) alogliptin, have been identified, accounting for less than 1% and about 5%, respectively. In the case of linagliptin, the parent compound accounts for about 70% of the drug-bound plasma material, while the major metabolite (CD 1790, S-3-hydroxypiperidinyl derivative of linagliptin) accounts for about 18% of the parent compound. The formation of CD1790, which is pharmacologically inactive, is CYP3A4 dependent. In addition, seven minor metabolites have been identified (each ranging from 0.3 to< 5% связанного с линаглиптином материала плазмы).
In contrast to the inhibitors described above, both vildagliptin and saxagliptin are extensively metabolized in humans (Table 2). The main metabolic pathway for vildagliptin is hydrolysis, which occurs in the liver and other tissues through a CYP450-independent mechanism to form carboxylic acid metabolites (M20.7 / LAY151) and four small metabolites. The parent molecule and the main metabolite, which is pharmacologically inactive, represent the main part of the plasma material associated with vildagliptin (about 22 and 55%, respectively). Saxagliptin is metabolized in the liver by CYP3A4 / 5 to form the main metabolite (5-hydroxy-saxagliptin, BMS-510849), which is also a competitive reversible inhibitor of DPP-4 with almost 50% potency compared to the parent drug. The parent molecule accounts for 22% of the saxagliptin bound plasma material, while BMS-510849 and other unidentified small monohydroxylated metabolites account for 76%.
Excretion
Usually, DPP-4 inhibitors are excreted primarily through the kidneys, and the rate of renal clearance exceeds glomerular filtration, which suggests the involvement of active transport in the process. For sitagliptin, about 70% of the dose is excreted unchanged, and it has been shown that active transport accounts for about 50% of its clearance. The following proximal tubule transporters have been identified to be involved: human organic anionic transporter (OAT) -3, organic anionic transport polypeptide (OATP) -4C1, and Pgp. Alogliptin (and its small metabolites) are excreted by the kidneys, and about 60 - 70% of the dose is found in the urine as the parent compound. Alogliptin clearance is greater than normal glomerular filtration, but renal transporters involved in the process have not been identified, although drug interaction studies suggest a low likelihood of Pgp involvement. Similarly, saxagliptin and its main metabolite (BMS-510849) are mainly eliminated by the kidneys, accounting for 24 and 36% of the dose, respectively. Again, the renal clearance of the parent compound exceeds the glomerular filtration rate, indicating that active renal secretion is being used, the mechanism of which is not known. It is known that saxagliptin is not a substrate for OAT1, OAT3, OATPA, OATPC, OATP8, organic cationic transporter (OCT) -1, OCT-2, sodium taurocholate cotransporter peptide or peptide transporters (PepT1 and PepT2). In contrast, the clearance of BMS-510849 is similar to glomerular filtration, suggesting that this is the primary elimination mechanism used. Data on vildagliptin also show that the kidneys are the main route of excretion, with 22% of the dose being in the urine unchanged and 50% as the main metabolite (M20.7). It has been shown that active transport, in addition to glomerular filtration, is involved in the elimination of both compounds.
Linagliptin is an exception, only< 6% дозы экскретируется с мочой. Это может отчасти быть связано с высокой степенью связывания с белками, означая что препарат избегает клубочковой фильтрации. Преимущественно линаглиптин имеет печеночный путь элиминации: 78 % дозы оказывается в кале в неизменном виде. Почечная экскреция основного метаболита (CD1790) ничтожна, он подвергается дальнейшему метаболизму и также выводится с каловыми массами .
Potential drug interactions
According to available data, DPP-4 inhibitors generally do not lead to any significant activation or suppression of the CYP enzyme system, which makes them unlikely to participate in clinically significant drug interactions involving this enzyme system. There is evidence of a low likelihood of a clinically significant interaction of DPP-4 inhibitors with other commonly prescribed drugs, including metformin, pioglitazone, rosiglitazone, glyburide and simvastatin, which indicates the possibility of their combined use without the need to adjust the doses of each drug.
As mentioned above, CYP3A4 / 5 are involved in the conversion of saxagliptin to its active metabolite (BMS-510849), and potent CYP3A4 / 5 inhibitors such as ketoconazole increase the exposure of the parent compound. For this reason, it is recommended to reduce the dose of saxagliptin by 50% (up to 2.5 mg / day) when administered together with strong inhibitors of CYP3A4 / 5. Linagliptin is also a substrate for CYP3A4, and ketoconazole prevents the formation of the CD1790 metabolite. However, since this metabolite is of only minor importance in the clearance of linagliptin, inhibition or induction of CYP3A4 by concomitant drugs does not significantly impair the overall effect of linagliptin. In addition, linagliptin is a weak competitive inhibitor of CYP3A4, leading to a decrease in the clearance of other compounds metabolized by this pathway by less than 2 times; linagliptin thus has a low potential for clinically significant interactions with drugs metabolized through this system.
Safety / portability
Some of the differences between DPP-4 inhibitors stem from preclinical safety studies and observations from a number of clinical studies.
Thus, there are reports that vildagliptin and saxagliptin, but not other DPP-4 inhibitors, are associated with unwanted skin toxicity in monkeys. However, this finding may be specific to monkeys, as this side effect has not been observed in other animal species in preclinical trials. It is also important that there are no reports of skin lesions in clinical trials for all DPP-4 inhibitors.
In the case of saxagliptin, a small, reversible dose-dependent decrease in absolute lymphocyte count was noted in several studies, but this was not observed for other DPP-4 inhibitors. The effect was more evident at doses of saxagliptin ≥ 20 mg (which is higher than the therapeutic dose), but the values \u200b\u200bremained within the normal range. There was no effect on leukocytes or neurophil count, and there was no evidence of impaired immune function. Currently, the clinical significance of this remains unclear.
During the registration period of vildagliptin, a meta-analysis of clinical data revealed that a single dose of 100 mg of the drug was associated with a slight increase in hepatic transaminases compared to placebo and a dose of vildagliptin 50 mg when taken twice. For this reason, the recommended therapeutic dose was changed to 50 mg 2 times a day, and this was accompanied by recommendations for the need to monitor liver function before the start of admission, every 3 months during the first year, and periodically thereafter. Subsequently, a trend towards a moderate increase (more than three times the upper limit of normal) liver enzymes was confirmed in a broader pooled safety analysis, but this was not associated with an increase in the frequency of truly adverse events from the liver. However, liver function testing is still recommended for vildagliptin and is not approved for use in patients with hepatic impairment.
Despite the observations described above, in general, DPP-4 inhibitors, as a class of antihyperglycemic drugs, are well tolerated and the frequency of the noted side effects was low and, in general, did not differ from placebo and comparison drugs. An early meta-analysis of incretin-targeted therapy (which included data for sitagliptin and vildagliptin only), however, indicated an increased risk of certain infections (urinary tract infections for both inhibitors and nasopharyngitis for sitagliptin) and headache (more so for sitagliptin). vildagliptin). Since then, updated safety analyzes (each for\u003e 10,000 patients lasting more than 2 years) of clinical trials with sitagliptin and vildagliptin have been published and have shown no increased risk of urinary tract infections, respiratory infections or headache, as well as no increased risk of other adverse effects. compared with placebo and comparison drugs. Recent debate about the potential link between antihyperglycemic drugs and cancer or bone fractures does not seem to extend to DPP-4 inhibitors, as there is no evidence for this in safety analyzes. The cardiovascular safety of new drugs, including antihyperglycemic drugs, is also in the spotlight, requiring confirmation that there is no increased cardiovascular risk for new drugs. Retrospective analyzes of clinical trial data have not shown an increased cardiovascular risk for all drugs in the DPP-4 inhibitor group, but large prospective studies designed specifically to evaluate the effects of these drugs on cardiovascular outcomes are still ongoing. Thus, the final results of the studies Carmelina (a placebo-controlled study on cardiovascular safety and renal outcomes with linagliptin therapy) and Carolina (direct comparison of linagliptin and glimepiride in relation to cardiovascular outcomes) are expected by 2017-2018. It is also actively debated whether incretin-targeted therapy, including the use of DPP-4 inhibitors, is associated with an increased risk of pancreatitis. So far, there has been no evidence of this from pooled safety analyzes and retrospective analyzes of large public health databases. However, long-term follow-up and continued vigilance are still needed to confirm these results.
Application in special clinical situations
Renal failure
Chronic kidney disease (CKD) contributes to an increased risk of hypoglycemic conditions due to decreased clearance of creatinine and some hypoglycemic agents, as well as impaired renal gluconeogenesis, which requires antihyperglycemic therapy to minimize these risks.
Since most of the described DPP-4 inhibitors are excreted through the kidneys, it is expected that impaired renal function may affect their pharmacokinetic profile. In light of this, the concentration of DPP-4 inhibitors in plasma increases proportionally according to the degree of renal failure. Based on the studies conducted, sitagliptin, vildagliptin and saxagliptin are approved for use in patients with mild renal function impairment (creatinine clearance 50 - 80 ml / min) without changing the dose if indicated. Sitagliptin and Saxagliptin can be prescribed to patients with moderate to severe renal impairment (creatinine clearance 30-50 ml / min and<30 мл/мин соотвественно) при соответствующей коррекции дозы (табл. 5). Алоглиптин также элиминируется через почки и может применяться у пациентов с умеренной и выраженной хронической болезнью почек при соответствующей коррекции дозы (табл. 5) . Поскольку 95 % линаглиптина экскретируется с желчью через пищеварительный тракт, то нарушение функции почек не оказывает существенного влияния на фармакокинетику этого ингибитора ДПП-4 . Более того, коррекции дозы линаглиптина не требуется даже в ситуации выраженной почечной недостаточности и у пациентов с терминальными стадиями ХБП .
Liver failure
Among the concomitant disorders in patients with type 2 diabetes, liver pathology is often found, in the structure of which non-alcoholic fatty liver disease ranks first (70%). In addition, type 2 diabetes is detected in 30% of patients with liver cirrhosis. This explains the high requirements for the safety of hypoglycemic therapy in patients with impaired liver function.
DPP-4 inhibitors are generally well tolerated by patients with impaired liver function, and liver failure has no clinically significant effect on the pharmacokinetics of these drugs. Most studies indicate that when used in patients with impaired liver function, dose adjustment of DPP-4 inhibitors is not required. In the case of vildagliptin, it is necessary to control the level of transaminases, and the drug is not recommended for use in patients with a level of transaminases more than 3 times higher than the upper limit of the norm before starting treatment. Also, since there is an increase in the plasma concentration of saxagliptin with impaired liver function, patients with moderate hepatic impairment should be prescribed saxagliptin with caution. In a clinical study in patients with type 2 diabetes and impaired liver function of varying severity, including acute cirrhosis with portal hypertension, linagliptin did not cause further deterioration of liver function, the frequency of side effects did not increase, and hypoglycemic reactions were not detected. Even in severely impaired liver function, dose adjustment of linagliptin is not required (Table 6).
Table 5. Restrictions on the use of DPP-4 inhibitors for impaired renal function [according to C.F. Deacon, 2011]
|
linagliptin |
saxagliptin |
sitagliptin |
vildagliptin |
|
|
no dose adjustment required |
no dose adjustment required |
no dose adjustment required |
no dose adjustment required |
|
|
Medium / moderate |
no dose adjustment required |
dose reduction by 2 times (2.5 mg 1 p / s) |
dose reduction by 2 times (50 mg 1 r / s) |
dose reduction by 2 times (50 mg 1 r / s) |
|
no dose adjustment required |
dose reduction by 2 times (2.5 mg 1 p / s) |
dose reduction by 4 times (25 mg 1 p / s) |
dose reduction by 2 times (50 mg 1 r / s) |
Table 6. Restrictions on the use of DPP-4 inhibitors in case of liver dysfunction [by C.F. Deacon, 2011]
|
Degree of decreased kidney function |
linagliptin |
saxagliptin |
sitagliptin |
vildagliptin |
|
Light degree |
no dose adjustment required |
no dose adjustment required |
no dose adjustment required |
no dose adjustment required |
|
Severe degree |
no dose adjustment required |
no dose adjustment required |
not researched |
Elderly patients
In the treatment of diabetes in elderly patients, it is necessary to prescribe antihyperglycemic drugs with a minimum risk of hypoglycemia. In addition, careful monitoring of renal function is necessary, since often normal blood creatinine levels are combined with a decrease in creatinine clearance (low GFR). In this regard, with prolonged use, hypoglycemic drugs are safer with minimal excretion through the kidneys, the metabolites of which are excreted mainly with bile through the digestive tract. The results of 7 placebo-controlled phase III clinical trials demonstrated that linagliptin is effective, well tolerated, contributes to the achievement of individual therapy goals, and also allows you to control the risks of hypoglycemic conditions in elderly patients with type 2 diabetes.
DPP-4 inhibitors since their inception have taken a firm place in the line of drugs for the treatment of type 2 diabetes. The low risk of hypoglycemia, no effect on body weight and the absence of side effects from the gastrointestinal tract distinguish this class from other oral antidiabetic drugs. Differences among gliptins relate to their chemical structure, ability to inhibit DPP-4, duration of their action, metabolism and elimination. At the same time, the data available to date indicate their identity in terms of sugar-lowering activity, safety and tolerability. Gliptins can be prescribed to patients with newly diagnosed type 2 diabetes, with poor tolerance or contraindications to the appointment of biguanides, and also in combination with other oral antihyperglycemic drugs. Linagliptin is a DPP-4 inhibitor with proven efficacy and high safety profile. Due to its unique pharmacological profile, linagliptin can be used in patients with renal or hepatic insufficiency of varying severity without requiring dose adjustment. In addition, good tolerance, a convenient regimen of intake and dosing, a low risk of hypoglycemia, and no negative effect on the risk of developing cardiovascular diseases make linagliptin the drug of choice in a wide range of patients with type 2 diabetes, including the elderly.
List of references:
1. Shestakova E.A., Galstyan G.R. Inhibitors of dipeptidyl peptidase-4: a comparative analysis of the representatives of the group // Problems of endocrinology. 2012; 1: 61-66.
2. Amori R.E., Lau J., Pittas A.G. Efficacy and safety of incretin therapy in type 2 diabetes: systematic review and meta-analysis // JAMA 2007; 298: 194-206.
3. Aroda VR, Henry RR, Han J et al. Efficacy of GLP-1 receptor agonists and DPP-4 inhibitors: meta-analysis and systematic review // Clin Ther 2012; 34 (6): 1247-1258.
4. Baggio L.L., Drucker D.J. Biology of incretins: GLP-1 and GIP // Gastroenterology 2007; 132: 2131-57.
5. Bailey T. Options for combination therapy in type 2 diabetes comparison of the ADA / EASD position statement and AACE / ACE algorithm // Am J Med 2013; 126: S10-20
6. Cox ME, Rowell J, Corsino L, Green JB. Dipeptidyl peptidase-4 inhibitors in the management of type 2 diabetes: safety, tolerability, and efficacy // Drug Health Patient Saf 2010; 2: 7-19
7. Deacon CF. Dipeptidyl peptidase-4 inhibitors in the management of type 2 diabetes: a comparative review // Diabetes Obes Metab 2012: 13 (1): 7-18.
8. DeFronzo R.A. From the triumvirate to the ominous octet: a new paradigm for the treatment of type 2 diabetes mellitus // Diabetes 2009; 58 (4): 773–95.
9. Golightly LK, Drayna CC, McDermott MT. Comparative clinical pharmacokinetics of dipeptidyl peptidase-4 inhibitors // Clin Pharmacokinet. 2012; 51 (8): 501-14.
10. Graefe-Mody U, Friedrich C, Port A et al. Effect of renal impairment on the pharmacokinetics of the dipeptidyl peptidase-4 inhibitor linagliptin // Diabetes Obes Metab. 2011; 13 (10): 939-46.
11. Graefe-Mody U, Rose P, Retlich S et al. Pharmacokinetics of linagliptin in subjects with hepatic impairment // Br J Clin Pharmacol. 2012; 74 (1): 75-85.
12. Holst J.J., Gromada J. Role of incretin hormones in the regulation of insulin secretion in diabetic and nondiabetic humans // Am. J. Physiol. Endocrinol. Metab. 2004; 287: 199-206.
13. Holst J.J. The physiology of glucagon-like peptide-1 // Physiol. Rev. 2007; 87: 1409–39.
14. McGill JB, Sloan L, Newman J et al. Long-term efficacy and safety of linagliptin in patients with type 2 diabetes and severe renal impairment: a 1-year, randomized, double-blind, placebo-controlled study // Diabetes Care 2013; 36 (2): 237-244 /
15. Schernthaner G, Barnett AH, Patel S et al. Safety and efficacy of the dipeptidyl peptidase-4 inhibitor linagliptin in elderl patients with type 2 diabetes: a comprehensive analysis of data from 1331 individuals aged ≥ 65 years // Diabetes Obes Metab 2014; 16 (11): 1078-86.
16. Seino Y, Fukushima M, Yabe D. GIP and GLP-1, the two incretine hormones: similarities and differences // J Diabetes Investig 2010; 1: 8-23.
17. Toft-Niesen M.B., Damholt M.B., Madsbad S. et al. Determinants of the impaired secretion of glucagon-like peptide-1 in type 2 dia betic patients // J. Clin. Endocrinol. Metab. 2001; 86: 3717-3723.
Catad_tema Type II diabetes mellitus - articles
Comparative evaluation of the clinical and economic efficiency of dipeptylpetidase-4 inhibitors in the treatment of type 2 diabetes mellitus
A.V. Sabanov, Volgograd State Medical University
ON THE. Petunin, Sechenov First Moscow State Medical University
N.V. Matveev, Russian National Research Medical University. N.I. Pirogova
A.V. Luneva, Takeda-Russia company
Gastroenteropancreatic hormones, incretins, glucone-like peptide 1 (GLP-1) and glucose-dependent insulinotropic polypeptide (GIP) are important components in the regulation of carbohydrate metabolism. They contribute to an increase in insulin secretion, suppression of glucagon production and, accordingly, a decrease in glycemic levels. Incretins also have a variety of additional pleiotropic effects. However, the action of GLP-1 and GIP is short-lived, since they are cleaved by the enzyme dipeptidyl peptidase (DPP-4). It has been shown that in type 2 diabetes mellitus there is an incretin defect that can be stopped by the administration of DPP-4 inhibitors. DPP-4 inhibitors, which are a new class of glucose-lowering drugs, prevent the destruction of incretins, increase their level to supraphysiological and thereby lead to a decrease in blood glucose levels. Their use in patients with type 2 diabetes mellitus (DM 2) led to a steady decrease in the concentration of glycated hemoglobin (HbA1c), fasting blood glucose, generally acting on the glycemic triad. It is noteworthy that stimulation of insulin secretion and suppression of glucagon production is carried out by a glucose-dependent mechanism.
DPP-4 inhibitors have not only a pronounced hypoglycemic effect, but also a high level of safety, since they have a low risk of developing hypoglycemic conditions and do not contribute to an increase in body weight. Therefore, DPP-4 inhibitors are currently considered one of the most promising drugs used in the treatment of diabetes mellitus 2. They can be used both as monotherapy and in combination with other antihyperglycemic drugs - metformin, sulfonylurea derivatives, thiazalidinediones, and also with insulin.
Despite the significant similarity of DPP-4 inhibitors in the severity of their therapeutic efficacy and safety profile, there are some differences in the properties of individual drugs of this class, in particular, with respect to some pharmacokinetic characteristics, such as absorption, metabolism, elimination, as well as in the duration of action. in the level of selectivity and the degree of inhibition of the DPP-4 enzyme.
It is likely that the above differences may have a certain clinical significance, primarily for patients with impaired liver and kidney function, as well as for patients with cardiovascular diseases. In addition, these differences can affect the clinical and economic characteristics of the use of these drugs.
In this regard, a comparison was made of the clinical and economic efficiency of five drugs in this group: alogliptin, registered in Russia in 2014 (Vipidia®, Takeda) and drugs already known in Russia - linagliptin (Trazhenta®, Bjehringer Inngelheim), saxagliptin (Ongliza® , Bristol-Myers Squibb), sitagliptin (Januvia®, Merck Sharp & Dohme), vildagliptin (Galvus®, Novartis). In 2014, only vildagliptin was included in the VED list; in 2015, saxagliptin and sitagliptin were added to this list. In order to compare the clinical characteristics of the above drugs as objectively as possible, we undertook a search for meta-analyzes comparing the clinical efficacy of various DPP-4 inhibitors. The total number of publications found in PubMed for the keywords "DPP4" and "meta-analysis" was 9, but of these, only one publication included an assessment of alogliptin, although it was devoted not so much to a comparison of efficacy as to the safety of various DPP inhibitors. 4.
A search for the keywords “meta-analysis” and “alogliptin” found 14 publications. In most of them, a simultaneous comparison of both the efficacy and the safety profile of individual members of the DPP-4 inhibitor class was not carried out. Such a comparison was most complete in one of the latest publications (Craddy P., Palin H.-J., Johnson K.I., 2014).
This study analyzed data on a range of efficacy and safety parameters for the following DPP-4 inhibitors: alogliptin, linagliptin, saxagliptin, sitagliptin, and vildagliptin. This meta-analysis was based on 85 publications describing the results of a total of 83 randomized clinical trials in which the studied drugs were used in patients with diabetes mellitus, both as monotherapy (14 studies) and in combination with other antihyperglycemic drugs such as metformin. , sulfonamide preparations and insulin.
Obviously, when assessing the efficacy and safety of combined antidiabetic therapy, it is more difficult to detect and compare differences in the efficacy of the studied DPP-4 inhibitors, taking into account the possible influence of other components of therapy.
In this regard, for pharmacoeconomic analysis, we used the data of the study by Craddy et al., Relating to monotherapy with DPP-4 inhibitors (Table 1). Patients with diabetes mellitus 2 who received any of the 5 compared DPP-4 inhibitors as monotherapy demonstrated a significant decrease in HbA1c levels compared with patients who received placebo.
Table 1.
Comparison of efficiency and safety indicators of DPP-4 inhibitors
| Index | Alogliptin | Linagliptin | Saxagliptin | Sitagliptin | Vildagliptin |
|---|---|---|---|---|---|
| The absolute change in HbA1c from the initial value,% | -0,58 (-0,83…-0,33) | -0,58 (-0,83…-0,35) | - 0,45 (-0,75… -0,15) | -0,59 (-0,75… -0,43) | -0,52 (-0,71…-0.31) |
| Absolute weight change, kg | -0,17 (-0,60… 0.23) | -0,12 (-0,62… 0,38) | - | 0,20 (-0,18…0,60) | 0,33 (-0,12…0,80) |
| Probability of hypoglycemia,% | 0,13 (0,0032…0,71) | 0,8 (0,0028.. 0,42) | 0,88 (0,062..3,8%) | 0,29 (0,046..0,97) | 0,37 (0,043-1,4%) |
| All indicators are presented as means with a 95% confidence interval. There were no significant differences between the indicators for different drugs (p\u003e 0.05) | |||||
Table 2.
Calculation of the annual cost of therapy with various DPP-4 inhibitors
The mean values \u200b\u200bof the change in body weight of patients taking various DPP-4 inhibitors did not differ significantly (despite a slightly more pronounced decrease in body weight when taking alogliptin and linagliptin), as well as the incidence of hypoglycemia when taking these drugs. All this made it possible to assess the indicators of the effectiveness and safety of these five drugs of the same group as comparable and to use the cost minimization method for pharmacoeconomic analysis. For this purpose, the cost of the course of therapy with each of the drugs was estimated per year.
Data on the average retail price of one package of linagliptin, saxagliptin, sitagliptin and vildagliptin in the third quarter of 2014 were obtained from the IMS Health Russia database. The maximum permissible selling price for the drug alogliptin was taken equal to 977.17 rubles (information provided by the manufacturer - Takeda company). Taking into account the size of the wholesale and retail markups for medicines included in the list of Vital and Essential Medicines used in accordance with the Decree of the Moscow Government dated February 24, 2010 No. 163-PP, the cost of alogliptin was 1,343.62 rubles. The calculation of the cost of annual therapy with each of the drugs, taking into account the average daily dose, the number of tablets in one package and the frequency of administration of the drug, is shown in Table 2.
Thus, therapy of type 2 diabetes with the use of alogliptin, with equal efficacy and safety, is 21% less expensive than therapy with linagliptin, 22% less expensive than vildagliptin, 44% less expensive than saxagliptin and 85% less expensive than with sitagliptin. LIST OF REFERENCES 1. Krentz AJ, Patel MB, Bailey CJ. New drugs for type 2 diabetes mellitus: what is their place in therapy? Drugs 2008, 68 (15): 2131–2162
2. Scheen AJ. A review of gliptins in 2011. Expert Opin Pharmacother. 2012, 13 (1): 81–99.
3. Esposito K, Cozzolino D, Bellastella G, et al. Dipeptidyl peptidase-4 inhibitors and HbA1c target of 4. Craddy P., Palin H-J, Johnson KI. Comparative Effectiveness of Dipeptidylpepti-dase-4 Inhibitors in Type 2 Diabetes: A Systematic Review and Mixed Treatment Comparison. Diabetes Ther., Jun., 2014, 5 (1): 1–41.
There are six types of tableted antihyperglycemic drugs, as well as their ready-made combinations, which are used only for type 2 diabetes:
-
Glitazones (pioglitazone)
Alpha glucosidase inhibitors
DPP-4 inhibitors
Sulfonamides
Combined
Biguanides (metformin)
Biguanides (metformin)
The biguanides include one drug called metformin. It has been used as a hypoglycemic drug since 1994. It is one of the two most commonly prescribed antihyperglycemic drugs (the other is sulfonamides, see below). It reduces the flow of glucose from the liver into the bloodstream and also increases the insulin sensitivity of insulin-dependent tissues. The tablets contain 500, 850 or 1000 mg of the drug. The initial dose is 1 table. (500, 850 or 1000 mg). After 10-15 days, the dose of the drug is increased by 1 table. if necessary. The maintenance dose is usually 1.7 g / day, prescribed 1-2 times a day, and the maximum dose is 2.55-3.0 g / day. It is usually taken 2 times a day, but there are long-acting medications that are taken once a day. It should be taken with or after meals. He enters the pharmacy chain under various names that manufacturers give him:
Baghomet (Bagomet ) (Argentina) - prolonged action, 850 mg / tab.
Glyformin (Gliformin ) (Russia, JSC "Akrikhin") - 500, 850 and 1000 mg / tab.
Glucophage (Glucophage ) (France) - 500, 850 and 1000 mg / tab.
Glucophage Long (Glucophage Long ) (France) - prolonged action, 500 mg / tab.
Siofor (Siofor ) (Germany) - 500, 850 and 1000 mg / tab.
Formetin (Formetin) (Russia, OJSC "Pharmstandard-Tomskkhimfarm") –500, 850 and 1000 mg / tab.
In addition to the fact that metformin lowers blood glucose levels, it also has the following positive qualities:
Low risk of developing hypoglycemia
Reduces the level of bad blood fats that predispose to atherosclerosis
Promotes Weight Loss
Can be combined with insulin and any other hypoglycemic drugs, if not effective enough on its own
Metformin also has undesirable (side) effects that should be discussed with your doctor if he prescribes metformin for you:
At the beginning of the appointment, it can cause diarrhea, bloating, loss of appetite and nausea. These phenomena gradually disappear, but when they appear, it is recommended to reduce the prescribed dose for a while until the indicated side effects disappear or decrease.
It should not be taken in case of renal failure, severe heart or pulmonary failure, liver disease. The drug should be discontinued in case of a sharp deterioration in metabolism, which requires hospitalization. Also, it should not be taken before an upcoming x-ray examination with iodine-containing contrast.
Cases of coma development (lactic acid) are described, when it was prescribed without taking into account contraindications
If you abuse alcohol, take certain heart medications, or are in your 80s, then metformin may not be for you.
With long-term use of metformin, there may be a lack of vitamin B 2, the manifestation of which must be monitored.
Glinides
Glinides include two drugs - repaglinide (Novonorm) and nateglinide (Starlix). These drugs stimulate the production of insulin by the pancreas. They are especially recommended for those with high post-meal blood glucose levels and are taken 3 times a day before each of the main meals. It makes no sense to combine them with sulfonamides, as they act in a similar way. In the pharmacy, they are presented under the names:
Starlix (Starlix ) (Switzerland / Italy, Novartis Pharma) - nateglinide 60 or 120 mg / tab. As a rule, the drug is taken immediately before meals. The time interval between taking the drug and eating should not exceed 30 minutes. When used as the only antihyperglycemic drug, the recommended dose is 120 mg 3 times / day. (before breakfast, lunch and dinner). If this dosing regimen fails to achieve the desired effect, a single dose can be increased to 180 mg. Correction of the dosage regimen is carried out on the basis of regularly, once every 3 months, the determined indicators of HbA1c and glycemia 1-2 hours after meals. Can be used in combination with metformin. In the case of Starliks \u200b\u200bjoining metformin, it is prescribed at a dose of 120 mg 3 times / day. before main meals. If, during treatment with metformin, the HbA1c value approaches the target, the dose Starlix may be reduced to 60 mg 3 times / day.
Novonorm (Novonorm ) (Denmark, the company "Novo-Nordisk") - repaglinide 0.5, 1.0 or 2 mg / tab. Initial dose composition it takes 0.5 mg if treatment with tableted antihyperglycemic drugs has not been previously prescribed or at a level HbA 1 c < 8%. Повышение дозы необходимо проводить не ранее, чем через 1-2 недели постоянного приема, но при печеночной недостаточности контроль осуществляется раньше. Maximum doses : single - 4 mg, daily - 16 mg. After using another hypoglycemic drug or at a level HbA 1 c ≥8% The recommended starting dose is 1 or 2 mg before each main meal. It is taken before main meals, usually 3-4 times a day. The optimal time for taking the drug is 15 minutes before a meal, but it can be taken 30 minutes before a meal or immediately before a meal. If a meal is skipped, then the drug is also not taken and, conversely, with an additional meal and the drug must be taken before it.
Unlike Starlix, Novonorm not only effectively lowers blood glucose after meals, but also lowers fasting blood glucose levels. On the other hand, Nateglinide causes hypoglycemic reactions to a lesser extent, but its effect on the level of HbA1c is also minimal. They are quite effective in the so-called "naive" diabetic patients with respect to sulfonamides. in those who have not previously received sulfa drugs.
In addition to the glucose-lowering effect, glinides have other positive qualities:
Does not cause weight gain.
To a lesser extent than sulfonamides cause hypoglycemia between meals and at night
The unwanted effects of clays include:
May cause hypoglycemia
Should not be taken for certain liver conditions
Glinides may be considered a starting therapy for T2DM, especially in individuals with an isolated increase in postprandial blood glucose and prefed blood glucose targets that are supported by diet and adequate physical activity. Candidates for treatment with glinides may be those who are afraid of developing hypoglycemia, in particular, elderly people. They are effective for those who rarely eat (1-2 times) during the day, but eat large portions. They can be used for allergy to sulfonamides, since they do not belong to them in chemical structure, and the mechanism of action is the same.
The sugar-lowering effect of glinides as a whole, which is assessed by the HbA 1c level, is 0.7-1.5%. Glinides can also be prescribed in combination with other hypoglycemic drugs, of course, with the exception of sulfonamides, with which they act in a similar way. For the same reason, one should not expect an effect from them in those whose sulfonamides have lost their effect or in those who are primarily insensitive to sulfonamides.
In general, the disadvantages of glinides are the need for multiple doses throughout the day, the low potential for HbA 1c reduction, and the high price.
Glinides can be prescribed for renal failure without any dose limitation. In persons with mild hepatic impairment, glinides are prescribed without restrictions, but their metabolism may slow down, which enhances the antihyperglycemic effect of glinides and their dose may be reduced or they may need to be administered at long intervals. They are contraindicated in severe hepatic impairment. They have no age restrictions.
Among the undesirable effects observed while taking glinides, hypoglycemia, upper respiratory tract infection, sinusitis, nausea, diarrhea, constipation, arthralgia, weight gain, and headache were noted.
Glitazones (pioglitazone)
Today, the only representative of this class of drugs is pioglitazone... It increases the insulin sensitivity of insulin-dependent tissues, and also reduces the production of glucose by the liver. In addition to lowering blood glucose, pioglitazone also improves fat metabolism. But at the same time, it also has negative properties:
Causes weight gain
Causes swelling
Increases the risk of developing heart failure
Increases the risk of developing fractures
In the pharmacy, this drug can be purchased under the names:
Aktos (Actos ) (USA, "Eli Lilly" company)
Diaglitazone (Diaglitazon ) (Russia, JSC "Akrikhin")
Tablets of any of the above preparations contain 15, 30 and 45 mg of pioglitazone . H assign inside 1 time / day. regardless of food intake. As the only drug, it is prescribed for those whose blood glucose target values \u200b\u200bhave not been achieved with the help of diet therapy and exercise and the initial dose in this case is 15 or 30 mg 1 time / day. If necessary, the dose can be gradually increased to 45 mg / day. If other antihyperglycemic drugs other than glitazone are not prescribed, then the maximum dose is 45 mg 1 time / day. If glitazone is combined with other hypoglycemic drugs (sulfonylureas or metformin), then glitazone is prescribed at a dose of 15 mg or 30 mg 1 time / day. At the beginning of treatment with glitazone, the sulfonylurea / metformin preparation can be left unchanged, and if hypoglycemia develops, the sulfanilamide / metformin dose must be reduced. In combination with insulin glitazone prescribed in a dose of 15 mg or 30 mg 1 time / day. At the beginning of drug treatment glitazone the insulin dose can be left unchanged. With the development of hypoglycemia and a decrease in blood glucose less than 5.5 mmol / l, the dose of insulin can be reduced by 10-25%. When glitazone is combined with other antihyperglycemic drugs, its maximum dose is 30 mg / day. Glitazone may be prescribed for renal failure.
Alpha glucosidase inhibitors
The mechanism of action of these drugs is that they interfere with the digestion of carbohydrates, that is, do not allow them to turn into glucose. Since only glucose can be absorbed, after taking carbohydrates with these drugs, blood glucose after meals does not increase or increases, but to a lesser extent. Thus, these medications are useful when blood glucose levels do not reach target values \u200b\u200bafter a meal. Obviously, if a person has taken glucose or sugary drinks (tea, coca-cola, sweets, etc.), then these drugs do not affect the increase in blood glucose in any way. Glucose doesn't need to be digested! But if a person ate potatoes and at the same time took this drug, then the blood glucose level after eating will rise less. They are especially useful in newly diagnosed type 2 diabetes where pre-meal glucose is in the target range and post-meal glucose is higher. Can be used in combination with any hypoglycemic drugs. Their main unpleasant action is associated with the effect on intestinal activity - they cause increased gas formation, diarrhea. This is why they should not be taken with metformin, which also disrupts bowel movements. In this combination, diarrhea and other very unpleasant sensations in the abdomen are guaranteed. Alpha-glucosidase inhibitors should also not be prescribed for bowel disease. However, they do not cause hypoglycemia. In the pharmacy, they are sold under the names:
Glucobay (Glucobay ) (Germany, Bayer) - the pharmacological name of the drug Acarbose, 50 or 100 mg in a tablet. The initial dose is 25-50 mg 3 times / day with the intake of carbohydrate-containing food. In case of insufficient effectiveness of treatment after 4-8 weeks of therapy, the dose can be increased to 200 mg 3 times / day. The maximum daily dose is 600 mg. Average daily dose of 300 mg (2 tablets of 50 mg or 1 tablet of 100 mg 3 times / day). The tablet should be taken whole, without chewing, with a little water, immediately before meals or chewed with the first serving of food.
Diastabol (Diastabol ) (Germany, Bayer company) - the pharmacological name of the drug Miglitol, 50 or 100 mg in a tablet. The initial dose is 25 mg 3 times a day with meals; if necessary, the dose is increased to 50 mg 3 times a day with an interval of 4-8 weeks; the maximum dose is 100 mg 3 times a day. It should be noted that although the drug is registered in Russia by BAYER AG in 1998 and is present in the Russian reference books of medicines (though without specifying the manufacturer and in the form of "Miglitol"), in clinical practice it is actually not used. On the Russian Internet, it is offered for purchase, but the Sites usually do not indicate the manufacturer, and if it is indicated, then not the company BAYER ... So, some caution should be continued with regard to its use in Russia.
DPP-4 inhibitors
DPP-4 inhibitors (IDDP-4) are a completely new class of hypoglycemic drugs that have been used in type 2 diabetes since 2006. In fact, they, by themselves, have no direct effect on insulin and its effect in the body. These drugs reduce the breakdown in the body of a substance like glucagon-like polypeptide 1 (GLP-1), which is produced in the intestinal wall in response to food intake. This is because they suppress (inhibit) the action of the DPP-4 enzyme, which destroys GLP-1. Hence their name - "DPP-4 inhibitors".
In turn, GLP-1 stimulates the secretion of insulin, and since under the influence of iDPP-4 there is more of it in the blood, this explains the hypoglycemic effect of iDPP-4. The sugar-lowering effect of GLP-1 is further enhanced by the fact that it inhibits the production of the hormone glucagon, which interferes with the action of insulin. DPP-4 inhibitors do not cause hypoglycemia, as they cease to act when blood glucose levels are normalized. They also do not cause weight gain and can be prescribed with any hypoglycemic drugs, except for injectable GLP-1 receptor agonists (see below), and only Galvus (vildagliptin) can be prescribed with insulin. Of the side effects - they cause discomfort in the abdomen, it is undesirable to prescribe them for certain diseases of the liver and kidneys. Today these are three classes of drugs - vildagliptin, saxagliptin and sitagliptin... They can be purchased at the pharmacy under the names:
Galvus (Galvus ) , (Switzerland, the company "Novartis") - vildaglpitin, tablets 50 mg. Galvus is taken orally, regardless of food intake. The usual recommended dose is 50 mg or 100 mg per day. But against the background of insulin treatment - 100 mg / day. A dose of 50 mg / day should be administered in one dose in the morning. A dose of 100 mg / day should be administered 50 mg 2 times a day, morning and evening. When combined with other tableted antihyperglycemic drugs, the Galvus dose is 50 mg / day in the morning once. In case of mild impairment of kidney and liver function, no correction of the dosage regimen is required
Onglyza (Great Britain, firms "Bristol-Myers" and "Astra Zeneca") – saxagliptin 2.5 and 5 mg / tab. It is prescribed once a day, regardless of food intake or as a single drug or with other tableted antihyperglycemic drugs. It is not used with insulin.
Januvia (USA, company "MSD ») – sitagliptin 100 mg / tab., Taken once a day, regardless of food intake.
Sulfonamides
Sulfonamides have been used as hypoglycemic drugs for a very long time (since the 1950s) and are the most commonly prescribed drugs. Their mechanism of action is that they stimulate the production of insulin by the pancreas. This effect was discovered by chance during the Second World War, when they were used to treat infections. They can cause hypoglycemia and also contribute to weight gain. Four classes of sulfonamides ( glibenclamide, gliclazide, gliquidone and glimepiride), which can be purchased at the pharmacy under the names:
Maninil 1.75 (Maninil 1,75) or Maninil 3.5 (Maninil 3,5) (Germany, firm "Berlin Chemie",) - glibenclamide in micronized form, 1.75 mg / table. or 3.5 mg / table. respectively. Maninil in micronized form is a high-tech, specially ground form of glibenclamide, which allows the drug to be absorbed faster.
1.75 is 1 / 2-1 tablet 1 time / day. In case of insufficient effectiveness, the dose of the drug is gradually increased until the daily dose is reached, which maintains the target glycemic level. The average daily dose is 2 tablets (3.5 mg). The maximum daily dose is 3 tablets (5.25 mg) and in exceptional cases - 4 tablets (7 mg). If it is necessary to take higher doses, switch to taking the drug Maninil 3.5. The initial dose of the drug Maninil 3.5 is 1 / 2-1 tablet 1 time / day. With insufficient effectiveness, the dose of the drug is gradually increased. The average daily dose is 3 tablets (10.5 mg). The maximum daily dose is 4 tablets (14 mg).
The drug should be taken before meals, without chewing and drinking a small amount of liquid. Daily doses of the drug, up to 2 tablets, should usually be taken 1 time / day. - in the morning, before breakfast. Higher doses are divided into morning and evening reception, that is, taken 2 times a day. If you miss one dose of the drug, the next pill should be taken at the usual time, while taking a higher dose is not allowed.
Maninil 5 (Maninil 5) (Germany, firm "Berlin Chemie",) - glibenkleamide (not micronized!) 5 mg / tab. The initial dose of the drug Maninil 5 is 2.5 mg 1 time / day. The sugar-lowering effect of the drug Maninil 5 develops after 2 hours and lasts 12 hours. With insufficient effectiveness under the supervision of a physician, the dose of the drug is gradually increased by 2.5 mg / day. with an interval of 3-5 days until the daily dose required to stabilize carbohydrate metabolism is reached. Increasing the dose of more than 15 mg / day. practically is not accompanied by an increase in the antihyperglycemic effect. Frequency rate of taking the drug Maninil 5 - 1-3 times / day The drug should be taken 20-30 minutes before meals. When transitionwith other hypoglycemic agents with a similar mechanism of action Maninil 5 is prescribed according to the scheme given above, and the previous drug is canceled. When switching from metformin, the initial daily dose is 2.5 mg, if necessary, the daily dose is increased every 5-6 days by 2.5 mg until compensation is achieved. In the absence of compensation within 4-6 weeks, it is necessary to decide on the conduct of combination therapy with tableted antihyperglycemic drugs of a different class or insulin (see T2DM treatment algorithms below). With an insufficient decrease in fasting glycemia, the dose can be divided into 2 doses - in the morning and in the evening with an interval of 12 hours (usually 2 tablets in the morning and 1 table in the evening).
Diabeton MV (D iabeton MR ) (France, firm "Servier") - drug gliclazide Modified Release (MB) 60 mg / table Firm "Servier" switched to the production of the drug at a dose of 60 mg / tab. instead of the previously produced dose of 30 mg / tab., and its production has begun in Russia (Moscow region). It is preferable to take the drug during breakfast - to swallow it whole without chewing or crushing. The drug is taken once a day.
The initial recommended dose for adults (including for the elderly ≥ 65 years) is 30 mg once a day (1/2 tablet 60 mg). In case of adequate control of diabetes, the drug at this dose can be used for maintenance therapy. In case of inadequate glycemic control, the daily dose of the drug can be sequentially increased to 60, 90 or 120 mg. If you miss one or more doses of the drug, you should not take a higher dose in the next dose, the missed dose should be taken the next day.
Increasing the dose is possible no earlier than after 1 month of drug therapy in the previously prescribed dose. The exception is cases when the blood glucose level did not decrease after 2 weeks of therapy. In such cases, the dose of the drug may be increased 2 weeks after the start of administration. The maximum recommended daily dose of the drug is 120 mg in 1 dose. 1 modified release tablet 60 mg is equivalent to 2 modified release tablets 30 mg. The presence of a notch on 60 mg tablets allows you to divide the tablet and take a daily dose of both 30 mg (1/2 tablet 60 mg) and, if necessary, 90 mg (1 tablet 60 mg and 1/2 tablet 60 mg). No dose adjustment is required for mild to moderate renal impairment.
Glidiab MV (G lydiab MR ) (Russia, JSC "Akrikhin") - gliclazide Modified Release (MB) 30 mg / tab. The rules for taking and dosing the drug are the same as for Diabeton MB.
Glurenorm (G lurenorm ) (firm "Boehringer Ingelheim") - glycidone 30 mg / tab. After taking the drug, the hypoglycemic effect develops after 1-1.5 hours, the maximum action is after 2-3 hours, the duration of action is 12 hours. The drug is administered orally at an initial dose of 15 mg (1/2 tablet) during breakfast, at the beginning of a meal.
Amaryl (A maryl ) (France, Sanofi firm) - glimepiride 1, 2, 3 or 4 mg / tab. The tablets should be taken whole, without chewing, with a sufficient amount of liquid (about 1/2 cup). The initial dose of the drug is 1 mg 1 time / day. If necessary, the daily dose can be gradually increased (at intervals of 1-2 weeks) in the following order: 1-2 -3 -4 -6 -8 mg per day. The effective dose of the drug does not exceed, most often, 4 mg / day. Dose over 6 mg / day. rarely used. The daily dose is prescribed in 1 reception, as a rule, immediately before a full breakfast or, if the morning dose has not been taken, immediately before the first main meal. There is no exact relationship between doses Amarila and other oral glucose-lowering drugs. When transferring from such drugs to Amaryl the recommended initial daily dose of the latter is 1 mg, even if transferred to Amaryl with the maximum dose of another oral antidiabetic drug. In case of insufficiently controlled diabetes mellitus while taking glimepiride or metformin in the maximum daily doses, treatment with a combination of these two drugs can be started. In this case, the previous treatment with either glimepiride or metformin continues in the same doses, and the additional intake of metformin or glimepiride begins with a low dose, which is then titrated depending on the target level of metabolic control, up to the maximum daily dose.
Glemaz (G lemaz ) (Argentina, firm "QUIMICA MONTPELLIER") - glimepiride 4 mg / tab. For instructions for use, see Amaryl.
Glimepiride (G limepiride ) (Russia, OJSC Pharmstandard-Leksredstva) - glimepiride 2, 3 and 4 mg / tab. For instructions for use, see Amaryl.
Diamerid (Diamerid ) (Russia, JSC "Akrikhin") - glimepiride 1, 2, 3 or 4 mg / tab. For instructions for use, see Amaryl.
Combined tablet preparations
In order to reduce the number of tablets taken, combinations of two antihyperglycemic drugs in one tablet were invented. There are preferred combinations of antidiabetic drugs. In particular, today it is recommended to prescribe metformin as a starting antidiabetic drug. As a result, it is metformin that turns out to be, as a rule, an obligatory drug for combined treatment. Hence, it is clear that modern combined drugs are metformin + some other hypoglycemic drug. So, in the pharmacy you can buy metformin in combination with the following drugs:
Metformin + Glibenclamide
Bagomet plus (Bagomet plus ) (Argentina, QUIMICA MONTPELLIER) - glibenclamide 2.5 / 5.0 mg + metformin 500 mg. Usually, the initial dose is 1 tablet of Bagomet Plus 500 mg / 2.5 mg or 500 mg / 5.0 mg once a day. If necessary, every 1-2 weeks after the start of treatment, the dose of the drug is adjusted depending on the level of glucose in the blood. When replacing the previous combination therapy with metformin and glibenclamide, 1-2 tablets of Bagomet Plus 500 mg / 2.5 mg or 500 mg / 5 mg (depending on the previous dose) are prescribed 2 times a day - in the morning and in the evening. The maximum daily dose is 4 tablets of the drug (500 mg / 2.5 mg or 500 mg / 5 mg, which is 2 g of metformin / 20 mg of glibenclamide). The tablets should be taken with meals.
Glibomet (G libomet ) (Germany , "Berlin-Chemie" company)- glibenclamide 2.5 / 5.0 mg + metformin 400 mg. The initial dose is 1-3 tablets / day. with further gradual selection of an effective dose until a stable compensation of the disease is achieved. The optimal regimen is 2 times / day. (morning and evening) with meals. The maximum dose is 5 tablets / day.
Glucovance (Glucovance ) (France, firm "MERCK SANTE") - glibenclamide 2.5 + metformin 500 mg. The initial dose is 1 tablet / day (2.5 mg / 500 mg or 5 mg / 500 mg). It is recommended to increase the dose by no more than 5 mg glibenclamide / 500 mg metformin per day every 2 or more weeks until the target glycemia is reached. The maximum daily dose is 4 tablets of the drug Glucovance 5 mg / 500 mg or 6 tablets of the drug Glucovance 2.5 mg / 500 mg. Dosage regimen for dosages of 2.5 mg / 500 mg and 5 mg / 500 mg:
1 time / day, in the morning during breakfast - with the appointment of 1 tablet per day;
2 times / day, morning and evening - with the appointment of 2 or 4 tablets per day.
Dosage regimen for dosage 2.5 mg / 500 mg:
3 times / day, morning, afternoon and evening - with the appointment of 3, 5 or 6 tablets per day.
Dosing regimen for dosage 5 mg / 500 mg:
3 times / day, morning, afternoon and evening - with the appointment of 3 tablets per day.
The tablets should be taken with meals. Each dose of the drug should be accompanied by a meal with a sufficiently high carbohydrate content to prevent hypoglycemia. Replacement of the previous combination therapy with metformin and glibenclamide: the initial dose should not exceed the daily dose of glibenclamide (or the equivalent dose of another sulfonylurea drug) and metformin, which were previously taken. In old age, the dose is set taking into account the state of renal function, which is regularly assessed during treatment. The initial dose for them should not exceed 1 tablet of the drug Glukovans 2.5 mg / 500 mg
Glukonorm(Russia, JSC Pharmstandard-Tomskkhimfarm) - glibenclamide 2.5 mg + metformin 400 mg. The usual starting dose is 1 tablet of Gluconorm 2.5 mg / 400 mg per day. Every 1-2 weeks after the start of treatment, the dose of the drug is adjusted depending on the blood glucose level. When replacing the previous combination therapy with metformin and glibeklamide, 1 - 2 tablets of Gluconorm are prescribed, depending on the previous dose of each component. The maximum daily dose is 5 Gluconorm tablets.
Metformin + Dliclazide
Glimecomb (Glimecomb ) (Russia, JSC "Akrikhin") - gliclazide 40 mg + metformin 500 mg. Take the drug swab inside during or immediately after meals, usually 2 times a day (morning and evening). The initial dose is usually 1-3 tablets / day. with a gradual selection of the dose until a stable compensation of the disease is achieved. The maximum daily dose is 5 tablets
Metformin+ Dlimpiride
Amaryl M (Amaryl M ) (Korea, the company "Handock Pharmaceuticals" ) - metformin 500 mg + glimepiride 2 mg (the form metformin 250 mg + glimepiride 1 mg is registered in Russia, but not yet supplied). It is recommended that you start at the lowest effective dose and increase the dose depending on your blood glucose level. In this case, appropriate monitoring of blood glucose levels should be carried out. The drug should be administered 1 or 2 times / day, before or during meals. In the case of a transition from combined treatment with separately taken tablets of glimepiride and metformin, the dose of Amaryl M should not exceed the doses of glimepiride and metformin that the patient received at this time.
Metformin + INsiltdagliptin
Galvus Met (Galvus Met ) (Switzerland, Novartis company) - tablets 50/500 mg, 50/850 mg and 50/1000 mg containing vildagliptin 50 mg + metformin 500, 850 or 1000 mg. When using Galvus Met, the recommended maximum daily dose of vildagliptin (100 mg) should not be exceeded. To reduce the severity of side effects from the digestive system, characteristic of metformin, Galvus Met taken with meals.
Initial dose of Galvus Met if treatment with vildagliptin alone is ineffective:galvus Met treatment can be started with one tablet with a dosage of 50 mg / 500 mg 2 times / day, and after evaluating the therapeutic effect, the dose can be gradually increased.
Initial dose of Galvus Met if treatment with metformin alone is ineffective: depending on the dose of metformin already taken, Galvus Met treatment can be started with one tablet with a dosage of 50 mg / 500 mg, 50 mg / 850 mg or 50 mg / 1000 mg 2 times / day
The initial dose of Galvus Met for those who previously received combination therapy with vildagliptin and metformin in the form of separate tablets:in depending on the doses of vildagliptin or metformin already taken, treatment with Galvus Met should be started with a tablet as close as possible in dosage to the existing treatment 50 mg / 500 mg, 50 mg / 850 mg or 50 mg / 1000 mg, and titrated according to the effect.
Galvus Met should not apply at renal failure or with impaired renal function ... When using the drug in patients over 65 years of age, it is necessary to regularly monitor renal function.
Metformin + Citagliptin
Janumet (Janumet ) (USA, company "MSD") - tablets 50/500 mg, 50/850 mg and 50/1000 mg Sitagliptin + Metformin. It is recommended to administer 2 times a day with meals, starting with the minimum dose and gradually increasing (titrating) to effective in order to minimize the gastrointestinal side effects of metformin.
If necessary, it is possible to gradually increase the dose to 120 mg / day. Further increasing the dose usually does not increase the effect. If the daily dose of Glurenorm does not exceed 60 mg (2 tablets), it can be administered in 1 dose during breakfast. When the drug is prescribed in a higher dose, the best effect is achieved when the drug is prescribed 2-3 times / day. In this case, the highest dose should be taken with breakfast. Though Glurenorm excreted in the urine is insignificant (5%) and is usually well tolerated in case of kidney disease, treatment of a patient with severe renal failure should be carried out under close medical supervision.

